Chylothorax secondary to thoracic duct malformation due to Klippel-Trénaunay syndrome. Case report
Gámez-Saiz, Ilse1; López-Ocampo, Paris Samahel1; Álvarez-Ramos, Karen1; Sánchez-Zazueta, Eduardo1

2024, Number 1
2024; 83 (1)


Gámez-Saiz, Ilse1; López-Ocampo, Paris Samahel1; Álvarez-Ramos, Karen1; Sánchez-Zazueta, Eduardo1
ABSTRACT
Klippel-Trenaunay syndrome is a rare congenital syndrome with an incidence of 1/100,000 cases per year caused by a sporadic somatic mutation in the PIK3CA gene. It is characterized by a triad of capillary malformations, abnormal growth of soft tissues and bones, usually affecting the lower extremities, and varicose veins in atypical locations. The presentation of chylothorax is rare, and few cases with high recurrence have been documented. The diagnosis of Klippel-Trenaunay syndrome is made through imaging studies to corroborate the malformations and genetic studies that demonstrate the somatic mutation. Regarding the diagnosis of chylothorax, analysis of the pleural fluid is required with a triglyceride result greater than 110 mg/dL. The treatment for chylothorax in the Klippel-Trenaunay syndrome is multidisciplinary, requiring support from nutrition, internal medicine and pulmonology to manage complications, as well as cardiothoracic surgery for definitive treatment.KEYWORDS
Klippel-Trenaunay syndrome, chylothorax, lymphatic malformations.Introduction
Klippel-Trénaunay syndrome (KTS) is a rare congenital syndrome with an incidence of 1/100,000 cases per year caused by a mutation in the PIK3CA gene, which has no sex or race predilection. It is characterized by a triad of capillary malformation, abnormal soft tissue growth, bone and venous malformation, usually affecting unilateral lower extremities. The presence of persistent embryonic veins represents the main vascular malformations in patients with KTS and there may be port wine stain presentation, other manifestations are hip dysplasia and syndactyly in up to 29% of cases; pulmonary manifestations debut with pulmonary hypertension secondary to emboli and pleural effusion, other pulmonary conditions are the development of chylothorax commonly secondary to a predisposing lesion or non-traumatic causes, which leads to high morbidity and mortality due to leakage of lymphatic fluid from the thoracic duct. The presence of chylomicrons with lipoprotein analysis and a triglyceride level of more than 110 mg/dL in the pleural fluid is sufficient for diagnosis.
Within the diagnosis of KTS, apart from the genetic study to document the gene mutation, patients should be studied with Doppler ultrasound and magnetic resonance imaging (MRI) to rule out arteriovenous fistulas with contrast phlebography, and to assess the degree of tissue hypertrophy and bone involvement. Treatment is always conservative, compression stockings can help improve pain and deformity of the affected limb, while sclerotherapy can be used to treat certain malformations. Regarding chylothorax, in the first instance, dietary adjustments should be made by changing the diet to short-chain triglycerides and considering parenteral nutrition; administration of drugs such as somatostatin may be used. Surgery is reserved for cases of previous failure of conservative treatment. The FDA (Food and Drug Administration) has recently approved the use of "alpelisib" a kinase inhibitor, which generates alterations in the cell cycle, especially on the PIK3CA mutation. The main causes of mortality are thrombotic events at pulmonary and cerebral level and infections.1-3
Clinical case
36-year-old male patient with a pathological history of KTS diagnosed at the age of three years through genetic study and angioresonance complementary to physical examination; history of hemangioblastoma in 2000 treated with radiotherapy, and supracondylar amputation in 2014 due to arterial thrombosis.
He began his current condition with dyspnea on minimal exertion, non-productive, non-cyanotic, breathless cough, exacerbated by changes in position; he went to a private unit where a diagnosis of pleural effusion with a macroscopic "milky" appearance was made. He was evaluated by the Pneumology area in our unit, which placed an endopleural probe with a total drainage of 1,500 cm3 of liquid of the same characteristics; subsequently, he was admitted for a chylothorax approach, which was drained again two weeks later.
Physical examination revealed a disseminated dermatosis on the right flank, gluteal region and stump on the right pelvic limb, consisting of a plaque of vascular neoformations, not confluent, wine-colored, no larger than 0.5 cm, raised, well demarcated, with areas of fine non-pruritic desquamation (Figure 1). Besides lymphostasis and significant hypertrophy of the left lower extremity with woody texture and extension to the scrotal region. The rest of the exploration only with presence of pleuropulmonary syndrome of pleural effusion.
Within the laboratory studies, white pleural fluid, milky appearance, cloudy, positive fibrin network, pH 8.5, density 1,020 mosm/kg, glucose 123 mg/dL, lactate dehydrogenase 109 IU/mL, protein 4.3 g/dL, albumin 2.6 g/dL, cholesterol 93 mg/dL, triglycerides 2,997 mg/dL, amylase 51 IU/L. General labs during his stay with hemoglobin 9 g/dL; leukocytes 7,000/mm3; platelets 650,000/mm3; urea 44 mg/dL; creatinine 1.3 mg/dL; glucose 120 mg/dL; sodium 140 mEq; potassium 3.4 mEq; Cl 100 mEq; cholesterol 210 mg/dL; triglycerides 158 mg/dL.
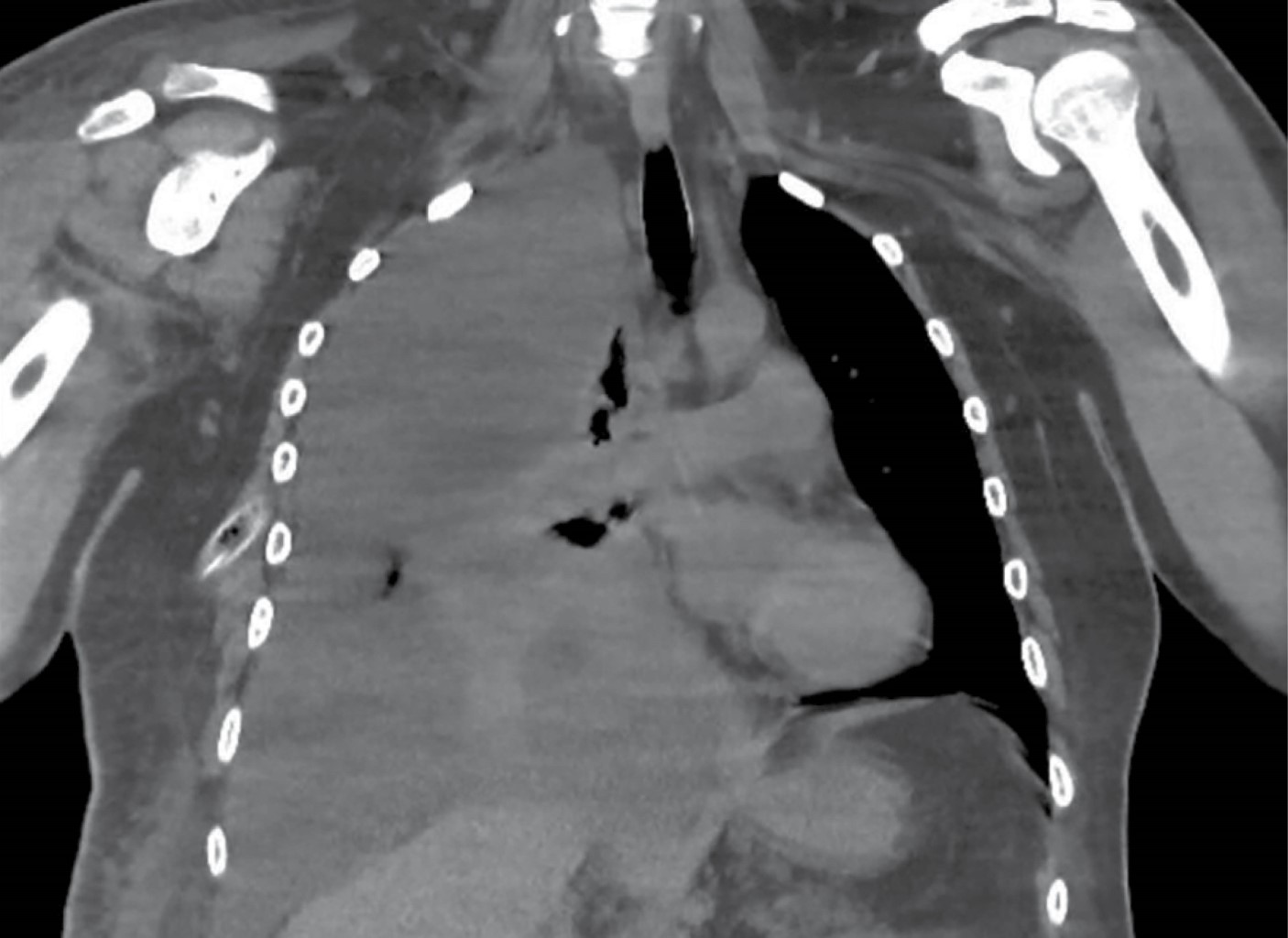
A simple computed tomography of the chest was performed with findings of pulmonary collapse, mild pericardial effusion, as well as mediastinal reactive lymph nodes (Figure 2). Adjustment of diet based on long-chain triglycerides was started for two months to reduce the production of chylothorax, management with octreotide 600 µg daily for two weeks and later with parenteral nutrition when there was no improvement. After three weeks, purulent material came out through the pleural drainage tube; it was decided to manage the patient with surgical cleaning and ligation of the thoracic duct in block with right pleural decortication by the Thoracic Surgery Service. There was evidence of a pleural effusion of approximately three liters with the presence of lax adhesions between the parietal and visceral pleura, pleural thickening varying from 2 to 5 mm and a dilated thoracic duct of approximately 7 mm. After the successful procedure and adequate re-expansion, chemical pleurodesis with iodopovidone was performed three times during hospitalization.
One week after the surgical event, with new formation of chylothorax, the patient was reintervened in cardiothoracic surgery; drainage, decortication and pericardial window were performed, and the aberrant thoracic duct was re-ligated. As a complication, he presented seroma of the surgical site, which was drained by placing a drenovac system; however, he had data of infection at the probe insertion site with a positive result for Acinetobacter baumannii. The patient continued with stabilization and improvement in the amount of pleural effusion in tomographic and radiographic controls, as well as remission of the infection. Pulmonary rehabilitation therapy was performed and he was sent home without recurrence of the chylothorax.
Discussion
Lymphatic manifestations are commonly seen in patients with KTS in the lower extremities, while in the thoracic manifestations only one case has been found in a young male patient with pulmonary disease, pleural and bilateral pericardial effusion. Thoracic malformations are commonly found in the retropleura and involvement of the posterolateral chest wall can trigger chyle leakage causing chylothorax. A broad search was carried out, finding only one case of KTS with recurrent chylothorax, in which drainage was performed with targeted videothoracoscopy with multiple areas of thoracic duct leakage; an excisional biopsy was performed on the posterior pleura, but inadvertently caused abundant chyle leakage requiring prolonged mechanical pressure with additional use of surgical adhesives (BioGlue®) and absorbable hemostatics (SURGICEL®) for control. PlasmaJet ablation of the parietal pleura was performed in an attempt to dry and seal remaining surfaces along with talc pleurodesis. Due to the pathogenesis of the disease, symptomatic drainage often fails, and definitive treatment must be instituted because of the increased risk of immunosuppression and malnutrition. Ligation of the thoracic duct is not recommended, mainly because of the overexpression of lymphatic collaterals due to the possible reflux of chyle to the lower body. In cases with significant leakage, modern local hemostatics may be effective and should be used instead of cauterization techniques; in chylothorax, restricted diet is helpful in decreasing chylothorax production, octreotide reduces the volume and duration of drainage quicker than with conventional management by itself; however, the optimal duration of treatment to assess response is still unknown. There are reports in neonatal patients of sirolimus for refractory chylothorax, with the only adverse effect being elevated liver enzymes. The target serum concentration is 10-15 ng/mL with a mean response time of 25 days.1,4-6
Conclusions
The relevance and importance of the diffusion of this case is the fact of secondary prevention of comorbidities that may occur, and the high rate of recurrence of lesions. Our patient already had a diagnosis of the disease, but the prevalence of the development of chylothorax as a manifestation of the underlying disease was unknown. As previously mentioned, there are no more than four cases reported about this in the literature and about its treatment; therefore, each case must be specified and adapted to the treatment options available in each medical unit. Fortunately, our patient is asymptomatic and without recurrence. It is important to consider that they present multiple hospitalizations and high risk of immunosuppression and infection, due to the same interventions, hospitalizations or the inflammatory and chronic underlying process.
AFILIACIONES
1High-Specialty Medical Unit, Specialty Hospital No. 2 "Lic. Luis Donaldo Colosio Murrieta", National Northwest Medical Center, Instituto Mexicano del Seguro Social. Ciudad Obregón, Sonora, Mexico.Conflict of interests: the authors declare that they have no conflict of interests.
REFERENCES
Mayer N, Perikleous P, De Rome K, Zhang YZ, Nicholson AG, Anikin V. A rare manifestation of Klippel-Trénaunay syndrome with bilateral chylothorax requiring surgical management—a case report. Curr Chall Thorac Surg [Internet]. 2022 Aug [cited: 2022 Aug 25];4:31-31. Available from: http://dx.doi.org/10.21037/ccts-20-111