Introduction
On January 1, 2020, the world learned of the emergence, in the city of Wuhan, of a new acute respiratory disease that showed signs of severity. From a distance, at that precise moment, we never had a clear picture of the global public health impact this disease, later known as COVID-19, would have.
Under the health emergency declared by the World Health Organization (WHO) on January 30, 2020, and the Strategic Preparedness and Response Plan published on February 3, all nations and their health systems had to work intensively on various relevant aspects; initially, to establish containment measures, perform rapid diagnosis through accurate tests, and evaluate and certify clinical laboratories to carry out large-scale testing in as many locations as possible for population care1. In Mexico, the National Epidemiological Reference Institute (INDRE) implemented the testing methodology and subsequently certified many clinical laboratories that today routinely perform the polymerase chain reaction test for SARS-CoV-2. The Microbiology Laboratory of the National Institute of Respiratory Diseases Ismael Cosío Villegas (INER) was one of the first in the country to implement and become certified for the test. On Thursday, February 27, 2020, the first COVID-19 case in Mexico was diagnosed at INER in a young man with acute respiratory symptoms who had recently visited Italy. The pace of activities to address the pandemic across the country was intense. Various policies, guidelines, recommendations, and protocols implemented by the Ministry of Health, published on the designated microsite2, resulted in activities in which health personnel played a central and transcendental role in outpatient and hospital care, as well as in implementing and monitoring disease prevention and containment measures throughout the population.
INER, as one of the hospital centers designated exclusively for COVID-19, transformed its patient care profile, medical facilities, and work protocols, from medical staff to administrative personnel. Throughout the pandemic, more than 5,000 patients were treated free of charge within the hospital, all of them critically ill and unfortunately, with a high mortality rate of 30%. In contrast, the majority of cases recovered successfully, continued with outpatient follow-up and rehabilitation, and were able to resume their daily activities.
All hospitals in the country under the same circumstances worked with the same intensity, facing new challenges and major problems. Opportunities to improve the healthcare system, and specifically respiratory medicine, are evident. The challenges are multiple and the variety of solutions is broad. As a starting point, and attempting to highlight the most relevant aspects, table 1 shows proposals that have been intensively analyzed and developed within INER. The challenges are broad, and the solutions are achievable because most of them already exist, but not in an integrated manner, so this presents a valuable opportunity to work for the benefit of our specialties with the ultimate goal of better comprehensive medicine.
Table 1. Challenges and solutions in respiratory medicine during a pandemic
| Challenges | Solutions |
|---|---|
| Best practices for outpatient and inpatient medical care | Diagnostic and treatment protocols Quality and safety of care Hospital reconversion Safe facilities Telemedicine |
| Healthcare worker safety | Occupational medicine Continuous training programs Personal protective equipment Optimization of medical profiles Universal vaccination |
| Sufficient and available health personnel | Needs planning Development of specialties and opening of training sites Training with future vision |
Best practices for outpatient and inpatient medical care
During the first year of the pandemic, the diagnostic protocol was fully standardized, and a large number of INDRE-certified laboratories became available throughout the country. Likewise, the pharmacological care of COVID-19 patients changed as more solid scientific evidence was generated, which showed poor or nonexistent clinical utility in resolving the infection for a list of drugs that are now definitively considered not recommended: ivermectin, azithromycin, hydroxychloroquine, stem cells, oseltamivir, transfer factor, chlorine dioxide, and several others. Unfortunately, outpatient care showed an overuse of these and even many other products with no or risky therapeutic utility. Treatment of outpatients who are not severe and not complicated should be limited exclusively to symptom control. In the case of severe patients requiring in-hospital treatment, several therapeutic regimens have been used in clinical trials, and with some of them, a decrease in mortality and hospital stay was demonstrated. The general recommendation is to use only drugs that have demonstrated their safety and efficacy in clinical trials. Patients discharged from the hospital should be followed under a multidisciplinary program and rehabilitation until full recovery. Furthermore, a number of patients with prolonged COVID-19 continue to require specialized care due to persistent symptoms or sequelae. In all cases, good medical practice requires following quality and safety guidelines fin patient care.
Hospital reconversion is one of the main strategies in case of a health emergency, as observed in other pandemics and as occurred with COVID-19. The need for hospital beds to care for severe cases can be enormous, so reconversion must include the largest possible number of beds, as well as changes in architectural and operational infrastructure, human resources, and necessary supplies2. If it is not possible to meet the cited requirements, safe reconversion cannot be achieved and, therefore, cannot be implemented. The case of INER is interesting because during the pandemic, the entire hospital reconversion process was completed progressively and in record time. This meant having 200 hospital beds equipped with mechanical ventilators, advanced vital signs monitors, and infusion pumps, as well as expansion of the medical gas network, which required the additional installation of two mobile liquid oxygen units with capacities of 19,000 and 23,000 liters (Figure 1), as well as the temporary hiring of more than 1,700 health workers and continuous management to have medications and supplies available. In addition, a field hospital was installed by the Mexican Red Cross, consisting of five interconnected tents, with independent installations of medical oxygen, air conditioning, electrical power, and its own staff to function as a critical care unit 24 hours a day.
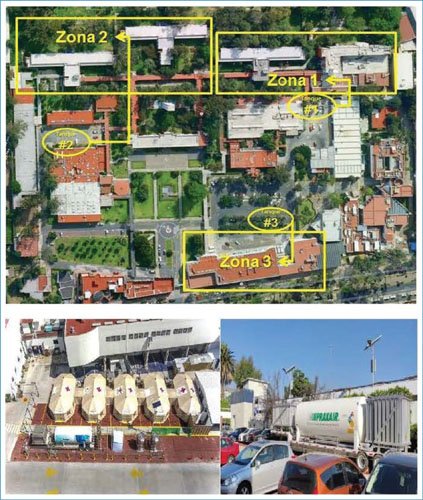
Figura 1. INER reconversion. Zona: zone; Tanque: tank.
Hospital reconversion requires continuous supervision and evaluation of all existing and newly implemented installations, with the purpose of maintaining optimal safety conditions; having safe installations guarantees the best care for critically ill patients and the well-being of healthcare personnel performing their work4. Some constant safety supervision activities include measuring medical gas pressure, reviewing electrical power conditions, determining water quality, measuring ambient temperature, monitoring the functionality of medical equipment, and microbiological analyses of clinical areas and medical instruments.
Telemedicine is the application of communication technologies to medicine, and this work methodology has advanced significantly in recent years. Communication by healthcare personnel with their peers, with families of hospitalized patients (tele- information), between hospitalized patients with their families (tele-visit), and with outpatients (teleconsultation), became a work routine5. Today, teleconsultation is more than ever, since in the face of a health emergency, it allows access and follow-up of people with chronic conditions. Obviously, it does not replace in-person consultation, but it does prevent distancing and certainly maintains communication with doctors and family members. The major challenge will be to further develop this form of communication, as the methodology must not only be implemented in the hospital network but also have the legal bases that support this form of medical care.
Healthcare worker safety
Among the most relevant priorities of the health system, everything related to patient care is of course paramount, but equally valuable is the care for the health, safety, and well-being of healthcare workers. This issue must always be a top priority. In pandemic conditions, it is an essential strategy to the irreplaceable and continuous work that healthcare workers perform for extended periods5. Additionally, staff health is more at risk than ever, and work shifts are exhausting, with great professional responsibility and often without rest or relaxation.
The most relevant action for INER healthcare personnel during the COVID-19 pandemic was the implementation of an occupational medicine unit with its own staff and within the hospital reconversion program. The main objective was immediate medical care, early diagnosis and treatment according to severity, hospitalization if necessary, or outpatient follow-up of mild cases; additionally, severe cases required rehabilitation and prolonged follow-up6. Physical health is compromised not only by the high risk of SARS-CoV-2 infection or any other infectious agent, but also by anxiety, depression, burnout, and uncontrolled chronic diseases, which were major health problems during the pandemic.
INER’s staff increased to 3,552 people in 2020; during just over the first year of the pandemic, 8,840 medical consultations were provided to these workers. Only 25% of positive cases were due to nosocomial transmission, some of them hospitalized, but the most relevant achievement is that there were no deaths among active personnel during the pandemic (Table 2). Other health problems in our healthcare staff included 80% anxiety, 70% depression, and 35% burnout.
Table 2. Results of INER’s occupational medicine program during the COVID-19 pandemic
| Parameter | December 2020 | January-March 2021 | ||
|---|---|---|---|---|
| Active personnel | 3,552 | 3,698 | ||
| Consultations provided | 8,480 | 1,504 | ||
| Positive cases | 518/3,552 | 14.58% | 134/3,698 | 3.62% |
| Nosocomial transmission | 122/518 | 23.55% | 0/134 | 0% |
| Community transmission | 396/518 | 76.45% | 134/134 | 100% |
| Hospitalized workers | 65/3,552 | 1.80% | 21/3,698 | 0.57% |
|
Deaths* |
5/3,552 | 0.14% | 0 | 0% |
*None among active personnel.
The continuous training program during the pandemic was a priority, mandatory, and continuous measure throughout the months. The objective was to inform hospital staff about the characteristics of the disease, transmission mechanisms, and prevention methods outside and inside their specific work environment. Training was provided to all workers, including new staff members, through the integration of a multidisciplinary group coordinated by the training department, who in turn supervised the personnel’s actions in situ. Training was both theoretical and practical, and updated throughout the months, specifically in the technique of donning and removing personal protective equipment and in the movement of people within the facilities (Table 3). Healthcare worker safety is only possible if there are availability and sufficiency of personal protective equipment according to each person’s performance. Consumption is very high (Figure 2), but it is an investment that translates into health and safety for workers, and the results demonstrated this. Incidentally, these measures apply to any type of pandemic or infectious outbreak, so training must be a constant activity in hospitals.
Table 3. Training program for INER health personnel during the first year of the COVID-19 pandemic
| Activity | Number of training sessions | Number of people trained |
|---|---|---|
| Personal protective equipment workshop-course | 317 | 3,612 |
| Videoconferences | 51 | 800,439 views |
| Educational videos | 10 | 328,714 views |
| Distance courses on COVID-19 | 9 | 1,311 |

Figure 2. Personal protective equipment and annual consumption during the COVID-19 pandemic.
The optimization of medical and nursing roles made it possible to offer the best care to patients and strengthened teamwork; for example, pulmonologists and intensivists in charge of all severe cases on mechanical ventilation, anesthesiologists dedicated to patient intubation, infectious disease specialists in charge of various specific drugs, surgeons performing tracheostomies and obtaining tissues in minimally invasive autopsies, otolaryngologists and researchers responsible for upper airway sample collection and institutional biosafety measures, internists with other specialties in triage and follow-up of outpatient cases, and teaching staff in organizing and delivering training, among others. The same occurred with nurses, even those incorporated into telemedicine follow-up of discharged patients with skin lesions and stomas. This teamwork generated empathy, cooperation, and professional solidarity among healthcare personnel.
Complete vaccination schedules must be guaranteed to all healthcare personnel, as has been done in previous years, and today different vaccines are incorporated for prevention against SARS-CoV-2. The ideal approach is always to have sufficient quantities of the best vaccines available and accessible to the entire population, including healthcare personnel, as a priority.
Sufficient and available health personnel
The COVID-19 pandemic revealed a significant shortage of healthcare personnel at all levels, and not only in Mexico, as this fact was observed worldwide. The challenge now is to achieve careful planning to cover this deficiency through the training of healthcare personnel across all areas, by analyzing the already established WHO standards for personnel sufficiency and the real needs of the country and health institutions.
The work of INER and all areas of respiratory medicine in the country should focus on concrete proposals, joint efforts, cooperation among hospitals, and strengthening our field of work. Two concrete proposals are the development of medical specialties and the opening of new training sites for specialist physicians. A well-known reality is the shortage of specialists in pulmonology and thoracic surgery. Mexico ranks very low among Latin American countries in terms of the number of specialists in these fields relative to the country’s population. For several years, this shortage has been analyzed, and growth proposals have been made that have not been consolidated7,8. In 2023, the Postgraduate Specialty in Pulmonology and Critical Care Medicine was created, thanks to the collaboration of specialists and the Councils of Critical Care Medicine and Pulmonology, and with the support of the authorities of the Faculty of Medicine of the National Autonomous University of Mexico. Only the University Hospital of Nuevo León has successfully trained physicians with this professional profile for several years, but the limited number of graduates does not significantly impact the country’s healthcare system. Healthcare institutions with the capacity to train this medical profile will be able to manage the opening of their training site, which will favor a substantial improvement in the number of specialists in a few years. The same process is required for training infectious disease physicians, intensivists, epidemiologists, nephrologists, and others, who were highly needed during the pandemic.
Future-oriented training must be the foundation for integrating the academic programs of new medical specialists; that is, with mastery of fields related to their specialty, solid training in clinical research, teaching, and ethics. The same approach should prevail for nursing. Of course, all this future planning for new personnel must be accompanied by balanced creation of job positions throughout the healthcare sector with dignified compensation. Achieving these goals is already a reality, as there are important higher education institutions capable of contributing, experts in all fields of medicine and nursing throughout the country, and interest from young people to be educated in these fields; so the conditions are in place, and now it is our responsibility to work for the country.
Conclusion
The experience of the H1N1 influenza and COVID-19 pandemics has shown that there are many opportunities for improvement, with the key lesson being the need to be prepared for future pandemics.
The new challenges of respiratory medicine and their new solutions are constantly evolving. Surely, what has been proposed in this article will soon be part of the daily routine; if this happens, we will have reached the fulfillment of our goals, and the cycle will repeat with new approaches.
Funding
None.
Conflicts of interest
The author declares no conflicts of interest.
Ethical considerations
Protection of people and animals. The authors declare that no experiments on humans or animals were conducted for this research.
Confidentiality, informed consent, and ethical approval. The study does not involve personal patient data and does not require ethical approval. SAGER guidelines do not apply.
Declaration on the use of artificial intelligence. The authors declare that they did not use any type of generative artificial intelligence for the writing of this manuscript.
