Definitions of pandemic
A pandemic (pan = all, demos = people) is an outbreak of disease for which humanity has no immunity, spreading across most or all of the world1. A more technical definition is “a worldwide epidemic or one occurring over a very large territory, crossing international borders and affecting a large number of people.” However, according to this definition, each winter influenza outbreak would be a pandemic, which is not the condition in which it is typically used. In the case of influenza, the occurrence of simultaneous outbreaks in both hemispheres, including an area outside the winter season, is what has most clearly characterized pandemics.
The formal definition applied by the World Health Organization (WHO) has been modified2; before 2009, an influenza pandemic was considered to occur when “a new influenza virus appears without human immunity, resulting in simultaneous epidemics worldwide, with an enormous number of deaths and illnesses.” Critics argued that the component of deaths and illness had been set aside, and that a pandemic could be declared for a worldwide outbreak that, according to some, was very mild. This additional concept of severity of the outbreak, unfortunately subject to discretion, somewhat delayed the declaration of the new SARS-CoV-2 pandemic3.
The influenza AH1N1 pandemic was declared on June 11, 2009, by the WHO, when the pandemic phase 6 definition was undoubtedly met, after determining that it was a new virus causing community outbreaks in at least two WHO regions. This phase-based definition does not take into account the severity of the outbreak nor an additional requirement previously considered, which was the transmission of a new viral variant (in influenza ta new hemagglutinin variant) and not an existing one with genetic components with a new reassortment among various species. In this classification, in phase 4, human-to-human transmission of a new and reassorted animal or human-animal virus is documented. Phase 5 additionally has sustained community transmission in two or more countries in the same WHO region, and phase 6 adds community transmission in an additional country from another WHO region. In general terms, based on what was previously stated, the following characteristics of a pandemic should be considered:
Caused by a new virus or pathogen without prior circulation in humans, implying null or minimal immunity.
Geographically widespread disease.
Person-to-person contagion and community spread.
In general, when referring of pandemics, explosive outbreaks are understood, not something that spreads slowly over years or decades.
Relatively high lethality, as opposed to infections that cause little discomfort or consequences.
Interestingly, COVID-19 met all these characteristics for a time before the pandemic was officially declared.
Historical pandemics
Pandemics have accompanied humans for millennia and most have been zoonoses, that is, diseases that originally have reservoirs in other animal species causing varying degrees of disease in them, and that at a given moment are transmitted to humans, when they achieve an adaptation that allows them to be transmitted among humans and spread. In contrast, as an example, in recent times there have been cases of avian influenza that have severely affected some humans with contact with birds, generating high lethality, but without the capacity to be transmitted among humans; the disease persists as isolated, exotic cases with pandemic potential if the virus were to adapt to transmission among humans.
The hunter-gatherer lifestyle of ancient humans, in groups with dozens of individuals, made it difficult for a disease to spread widely throughout the world, even the inhabited world at the time. Under these conditions, it is expected that an equilibrium would be quickly achieved between humans and microorganisms. Therefore, an indispensable factor for the existence of pandemics was the development of agriculture, with sedentarism and urbanization, and agglomerations of thousands of people who can easily transmit infections among themselves. Urbanization necessarily brings the need to trade goods, even at considerable distances, which allows an outbreak to spread. Finally, raising domestic animals, especially in herds, increased the possibility of evolution of pathogens for both humans and domesticated animals.
New population expansions were accompanied by new epidemics, such as that of the Mongols associated with the plague or Black Death, which caused a substantial loss of in the Old World population, and that of colonized America, lacking herd-type domestic animals, with catastrophic consequences due to the conquistadors becoming vectors of uncontrollable diseases at the time4. In this regard, pathogens and pandemics have been involved in historical events since their emergence. A classic example is smallpox in the New World, brought by the conquistadors, unknown in Mexico and causing 20-30% mortality in Tenochtitlán, including Emperor Cuitláhuac, which significantly contributed to the conquest.
The Industrial Revolution accelerated urbanization, just as the locomotive and steamships accelerated the speed of transport, facilitating the movement of people, microorganisms, and epidemics. Likewise, there was better coverage of their development by the press5, especially after the widespread use of the telegraph. Today, urbanization is a dominant global phenomenon and the speed of air transport allows an infection to take only a few days to spread throughout the world, even before there is awareness of a new infection. Air transport exponentially accelerates the spread of people, viruses, and outbreaks, following air routes; several pandemics, including COVID-19, have followed commercial flight routes.
The WHO has specified the requirements for a pandemic to emerge at present: 1) a new pathogen to which the population has no immunity, 2) capable of generating severe disease or death, and 3) capable of transmitting from person to person efficiently.
Pandemic models
In the mechanistic model of a pandemic, commonly called SIR (Susceptible, Infected, and Recovered) (Fig. 1), the epidemic ends only when the group of susceptible inhabitants disappears, either by having had the infection or by having received active or passive immunity. These population components would be the immediate causes of an infection and a pandemic, as well as its decline and disappearance. It has long been known that the characteristics of the germ are important for the development of infections, especially true for pandemics, but the characteristics of the pathogen, the human host, society, and, where applicable, the vector must also be considered (Fig. 1). It is equally important to consider that recurrent pandemics are not, as one might think, unconnected events, and therefore it is important to analyze factors common to their appearance that explain their recurrence, without which preventing them would be impossible.
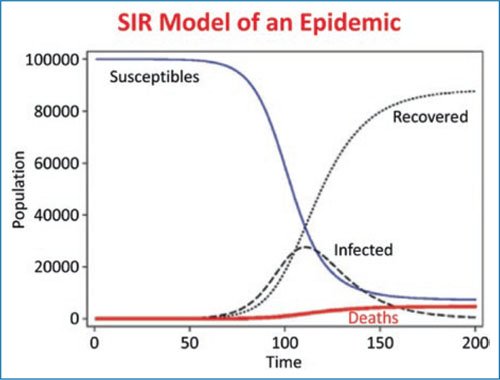
Figure 1. Typical SIR model (Susceptible, Infected, and Recovered) of an epidemic outbreak. The outbreak ends when susceptible population is depleted, either through infection or vaccination.
Causal factors of pandemic outbreaks and emerging diseases
Figures 2 and 3 describe the factors that should be considered in a pandemic, in addition to the presence of a new or modified pathogen that can be efficiently transmitted from person to person through an adaptation process.
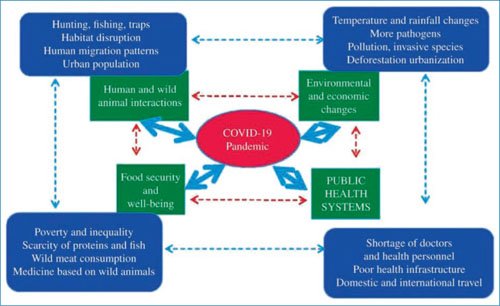
Figure 2. Factors involved in the COVID-19 pandemic (modified from Khan and Sesay [2015]7, from a conceptual model for the Ebola virus).
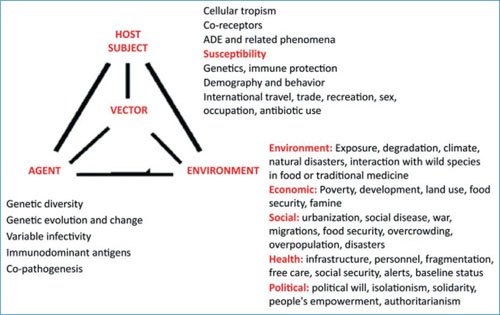
Figure 3. Relevant components of the agent, the host, and the environment for the generation of an infection, an outbreak, and a pandemic.
As can be seen, the factors include several that are not usually contemplated, such as urbanization, overcrowding, agglomerations, and global transport, identified for the SARS-CoV-2 pandemic, and which mostly apply to other pandemics and are the common thread of their recurrent appearance6,7.
Disruption of wildlife habitats
The expansion of areas inhabited by humans and urban sprawl displaces other species on one hand, confining them to increasingly smaller areas, and on the other hand increases the possibility of human interactions with wild species, which can be sources of infections. In COVID-19, the natural habitat of SARS-CoV-2 has been considered to be the bat. The spillover to humans of endemic viruses in bats or other wild species implies close contact between both species, as well as possible intermediate hosts. In SARS, the civet was considered an intermediate host, in MERS the camel, and in COVID-19 the pangolin was most frequently mentioned, although uncertainties remain. For influenza, pigs and various types of birds can serve as the source.
Climate change or global warming
The presence of extreme temperatures and catastrophic weather events, including both droughts in some areas and extreme rains with floods, promote adverse health conditions. Food scarcity may force inhabitants to enter zones of greater risk of zoonotic infections. Climate changes can also favor the growth of certain pathogens or vectors, and cause famines and migrations that force entry into contact with wild animals or their use as food or for traditional medicine.
Health systems that have not prepared for pandemics
Pandemics occur periodically, and despite this, the usual approach is to do everything possible to manage the outbreak, but in general nothing or almost nothing to be better prepared for the next pandemic, offering greater resources, such as doctors and health personnel, hospitals, hospital beds (especially intensive care for critically ill patients), primary care, reserve of ventilators, medical supplies, medications, and personal protection equipment, among others. Systems for identifying outbreaks and alerts to the population are also required.
Poverty, inequity, and overpopulation
These components make the search for food and the invasion of protected areas and wildlife habitats, which can transmit diseases, more common.
In summary, humanity frequently interacts with nature in an aggressive and harmful way. Fundamentally, this is the common causal factor of pandemics and other health emergencies.
Emerging diseases
More than 300 emerging disease events have been reported in recent decades, with a peak in the 1980s. These include zoonoses (60%) and resistant bacteria (54%), but also viruses and prions (24%), protozoa (10.7%), fungi (6.3%), and helminths (3.3%). Of these, 22% are transmitted by vectors and 21% are drug-resistant. Their origin correlates with socioeconomics, ecology, geography, or the environment, and they are geographically concentrated in so-called “hot spots,” at low latitudes with little or no epidemiological surveillance. As in pandemics, risk factors that have been invoked are virus adaptation and change, human susceptibility to infection, climate and climate change, ecosystem modification, human population behavior including overpopulation and population density, economic development and land use, international travel and trade, public health measures and their breakdown, poverty and social inequity, war and famine, lack of political will, and the intention to harm in the case of biological warfare. Emerging diseases have also been associated with the presence of rich and varied wildlife in the case of wildlife zoonoses, especially in epidemiologically poorly monitored areas where more economic resources should be concentrated, because they are sites with high probability of outbreaks of new or re-emerging infectious disease.
Table 1 summarizes the main emerging and re- emerging respiratory viruses, although there may be outbreaks of respiratory failure of non-infectious origin from inhalation of toxic substances, such as in industrial accidents.
Table 1. Emerging or re-emerging respiratory viruses
| Classical | New |
|---|---|
| Rhinovirus (> 100 variants) Parainfluenza 1, 2, 3 Respiratory syncytial virus A, B Adenovirus 14 (and > 50 variants) Endemic coronaviruses 229E, OC43 Enterovirus (> 10 variants) Hantavirus Influenza AH1N1, AH3N2 |
Parainfluenza 4 Metapneumovirus Rhinovirus C, D Torque teno virus High pathogenicity coronaviruses NL63, HKU1, SARS, MERS, SARS-CoV-2 Bocavirus Polyomavirus KI, MU? Influenza H1N1-2009 Avian influenza H7N7, H7N9, H10N8, H5N1, H10N7 and others New enteroviruses |
For further reference, the factors for the emergence or re-emergence of respiratory viruses and other infectious agents are described in the text.
Contributors to the origin of SARS-CoV-2 and COVID-19: a recent example
The Lancet Commission8 issued relevant opinions on the origin of the COVID-19 pandemic that are also applicable to the origin of other pandemics9. The first aspect is that it is an emerging zoonotic disease, with recombination of coronavirus genes within animals. This mechanism is common and has occurred in the influenza virus, the human immunodeficiency virus, SARS, MERS, Zika, Ebola, and others. The primary factor is increased contact between humans and animal reservoirs due to deforestation, soil degradation, poverty, or food insecurity, which forces populations to invade animal habitats. The Lancet group considered a probably natural origin rather than one deliberately created or escaped from a laboratory, although they insisted that rapid collaborative research be conducted.
By the time COVID-19 emerged, alerts had already been issued considering the situation to be high risk, with written statements indicating that the large reservoirs of coronaviruses in bats, similar to SARS, should be considered a time bomb, and that the possibility of SARS re-emergence and other new viruses from these reservoirs should not be ignored10,11. In this regard, several preventive activities are relevant and should be widely adopted12,13 (Table 2).
Table 2. Interventions that could prevent or reduce zoonotic and pandemic events
| Care for conservation areas Protect endangered species Prevent deforestation and mitigate climate change Monitor zoonotic events Monitor animal trade Monitor meat production and markets Ensure food security to avoid the need to hunt or rely on wild species Strengthen health systems including prevention, primary care, and referral centers for critically ill patients Reduce poverty, inequity, famines, and wars, and eliminate biological weapons Continue investigating the origin of SARS-CoV-2 and other pandemic viruses to incorporate additional mechanisms for pandemic prevention |
Cold weather and respiratory pandemics
Temperature and humidity considerably affect the stability and transmissibility of several respiratory viruses. The adverse impact of cold has been known for many years, since the name “influenza” derives from influenza di freddo (influence of cold). Many hypotheses have been put forward about the reason for this impact, such as the reduction in ultraviolet rays with decreased viral inactivation, the reduction in production and levels of vitamin D and melatonin in winter, as well as overcrowding and poor ventilation when seeking shelter from the cold. The most probable mechanisms in facilitating viral infections are low air temperature, low humidity content and its impact on the stability or survival of viral particles in the air; and also the dryness and cooling of the respiratory mucosa, which considerably affect the mucociliary defense mechanism and in extreme forms cause disruption of the respiratory mucosa. Empirical studies have shown that environmental cooling in winter increases the spread of influenza, respiratory syncytial virus, and seasonal coronaviruses. The SARS virus showed seasonality, and initial studies showed that COVID-19 prevalence in the United States of America and other countries was lower in areas that had more hours of sunlight, high temperature, and less cloudiness.
Expansion of the concept of pandemic to non-communicable diseases
In recent times, population growth, prolonged survival, aging, and air pollution, among other factors, in addition to harmful advertising that incites the consumption of ultra-processed foods, tobacco and alcohol, as well as sedentarism, have generated a progressive increase in some non-communicable diseases. Obesity, diabetes, cardiovascular and cerebrovascular diseases, chronic obstructive pulmonary disease (COPD), and a variety of malignant diseases, which have gradually become prevalent as causes of death, disease, and disability, have reached the point where epidemics or pandemics are being discussed. For example, smoking causes an estimated 8 million deaths per year worldwide, and users exceed one billion, with a greater number exposed to secondhand smoke and nicotine products. One can speak of a pandemic of smoking, obesity, or diabetes, if the requirement that it be an infectious disease is eliminated14,15. The WHO refers to global epidemics when discussing smoking and other non-communicable diseases, rather speaking of pandemics, although for practical purposes a global epidemic could be considered a pandemic. These new global epidemics or pandemics have collided adversely with infectious diseases, in what has been called a “syndemic”16. In the case of COVID-19, several of these diseases were shown to have more serious consequences from infection, in addition to aging; for example, diabetes, obesity, vascular diseases, and malignant neoplasms. Smoking directly interferes with respiratory tract defense mechanisms, and also generates varied systemic comorbidity, such as COPD, cardiovascular diseases, and neoplasms, and it has become increasingly clear that it also increases the risk of developing diabetes and obesity, and therefore worsens the prognosis of COVID-19, influenza, and other respiratory infections.
Evolution of influenza and COVID-19 pandemics
Both infections have evolved since the start of the pandemics, generating cases with lower mortality and fewer complications as a result of natural immunity in people who became ill and immunity from vaccinations. In addition to reduced infections throughout the year, seasonal outbreaks have occurred in winter, between November and April, especially in the United States of America and Europe, which has been attributed to greater survival of viruses in cold, humid air and to behavioral changes that favor contagion, as previously described17–19. It also highlights the need to reinforce immunity against SARS-CoV-2 before winter, as is customary for influenza, or throughout the year in places that do not exhibit a clear seasonal pattern. Outbreaks of various respiratory viruses (Table 2) have also emerged, including rhinovirus, seasonal coronavirus, parainfluenza virus, respiratory syncytial virus, adenovirus, metapneumovirus, and influenza A and B viruses, especially following the discontinuation of preventive measures implemented for COVID-19. These viruses occur regularly, and their clinical differentiation from influenza and COVID-19 is difficult or impossible, so virological surveillance is essential.
General reflection regarding pandemics
Pandemics have appeared periodically and will continue to appear, since they are not isolated phenomena, but derive from the complex and aggressive manner humans interact with the environment.
Harari20 reflected on several issues arising from COVID-19, which have been shared by other authors21, beginning with the idea that the current pandemic changed the world forever. The dilemmas he posed regarding the onset of COVID-19 are relevant, such as privacy versus health and isolation versus solidarity20.
It is also relevant that international collaboration and solidarity are required to generate a faster and more effective response to emerging and re-emerging situations22, and to minimize the manifestations of nationalisms observed in many places, such as hoarding of drugs and vaccines. Some solidarity efforts are also observed in parallel, such as sharing information and vaccine distribution mechanisms, such as COVAX, although with heterogeneous results. Harari20 rightly emphasizes that a great advantage we have against viruses is that we are capable of sharing information, but we must take maximum advantage of it. He also insists that solidarity begins in the immediate environment, in the neighborhood, the city, and the country, so it is totally illogical to expect international solidarity when it is not occurring in the local environment.
Pandemic preparedness
Pandemics have impacted society in multiple ways, highlighting the importance of preparation and investment in security measures to reduce the impact of future health crises23,24. After a pandemic passes, there is a tendency to react as if it were the last. The health system is not strengthened, which may remain fragmented, poorly funded, with few personnel, lacking self-sufficiency in supplies such as personal protective equipment, vaccines, mechanical ventilation systems and critical patient care, without timely warning systems, and without improving health information systems25. Public health infrastructures and surveillance capacity for detection, monitoring, and management of emerging outbreaks need to be strengthened26. National pandemic preparedness plans should be developed and then periodically reviewed and updated, to incorporate technological and scientific advances that improve detection and mitigation capacity27,28.
Funding
None.
Conflicts of interest
The authors declare no conflicts of interest.
Ethical considerations
Protection of people and animals. The authors declare that no experiments were performed on human beings or animals for this research.
Confidentiality, informed consent, and ethical approval. The study does not involve personal patient data nor does it require ethical approval. SAGER guidelines do not apply.
Declaration on the use of artificial intelligence. The authors declare that they did not use any type of generative artificial intelligence for the writing of this manuscript.
