Introduction
Pneumomediastinum and subcutaneous emphysema are uncommon complications that may occur during the peripartum period, with an estimated incidence of 1 in 100,000 deliveries. These conditions are frequently associated with prolonged labor and sustained, intense Valsalva maneuvers, which cause a significant increase in intrathoracic pressure1,2. Clinical presentation typically includes chest pain and dyspnea, as well as crepitus on palpation of the affected areas. Chest radiography is, in most cases, an adequate diagnostic tool for
identifying pneumomediastinum and subcutaneous emphysema. Characteristic findings result from air accumulation separating mediastinal structures and the thoracic wall3. Typical radiographic signs include the “continuous diaphragm” sign, the “double bronchial wall” sign, and the “Ginkgo leaf” sign. In addition, air may disseminate through fascial planes to the chest wall, abdomen, head, neck, and extremities, highlighting the notable capacity of these conditions to spread. Chest computed tomography (CT) is superior in terms of diagnosis, localization, and assessment of extent, as well as in establishing the differential diagnosis4.
This complication is usually benign and self-limited. Nevertheless, in rare cases, severe complications may occur, such as significant dyspnea and malignant pneumomediastinum requiring surgical intervention5,6. Although uncommon, these complications underscore the need for meticulous monitoring during labor and the postpartum period, particularly in patients with predisposing risk factors.
We report the case of an 18-year-old woman who developed pneumomediastinum and subcutaneous emphysema following a prolonged labor. Her hospital course was uncomplicated, and she required only conservative management.
Case report
An 18-year-old woman with no relevant family history or chronic medical conditions, prior hospitalizations, or surgeries was admitted. She was a primigravida at 40.3 weeks of gestation according to her last menstrual period and 40 weeks based on crown-rump length measurement. Her pregnancy was uncomplicated, and prenatal care was adequate. She was admitted due to increased uterine activity, with 6 cm cervical dilation, 80% effacement, bulging amniotic membranes, and a Bishop score of 11. Estimated fetal weight by the Johnson method was 3,100 g. Laboratory results were as follows: hemoglobin 13.4 g/dL, hematocrit 38.8%, platelets 137 × 103/µL, leukocytes 9.1 × 103/µL, prothrombin time 10.5 seconds, partial thromboplastin time 25.8 seconds, glucose 79.2 mg/dL, creatinine 0.56 mg/dL, HIV nonreactive, and VDRL nonreactive.
Labor induction was initiated with oxytocin, with a total labor duration of 7 hours. Full dilation and effacement were achieved 6 hours after admission. During labor, a specific maneuver was performed, placing the patient partially in the lithotomy position. A sheet was used so that the patient could pull on it while a staff member provided resistance, thereby increasing pushing effort. After 1 hour, the patient was transferred to the delivery room for vaginal birth. During the expulsive phase, a mediolateral episiotomy was performed after infiltration with lidocaine 20%. Due to ineffective contractions, the patient later reported that the Kristeller maneuver was performed, resulting in abrupt fetal expulsion.
An intrapartum complication included extension of the episiotomy repair toward the posterior fornix, approximately 5 cm in length, which was adequately repaired during the same procedure. The newborn measured 49 cm and weighed 2,895 g, with Apgar scores of 6 and 9, a Silverman-Anderson score of 3, and a Capurro score of 40. Due to signs of respiratory distress unresponsive to initial resuscitation maneuvers, continuous positive airway pressure was administered, and the newborn was admitted to the neonatal intensive care unit.
In the immediate postpartum period, subcutaneous emphysema was identified in the anterior chest region, right hemineck, and right submaxillary area. The patient was hemodynamically stable: heart rate 95 beats/min, blood pressure 130/87 mm Hg, respiratory rate 22 breaths/min, temperature 36.5 °C, and oxygen saturation 92%. At 48 hours, chest CT revealed spontaneous pneumomediastinum with extension of air into the pericardial space, predominantly in the right hemithorax, as well as dissection of tissue planes toward the right neck, clinically manifesting as cervicothoracic subcutaneous emphysema (Fig. 1).
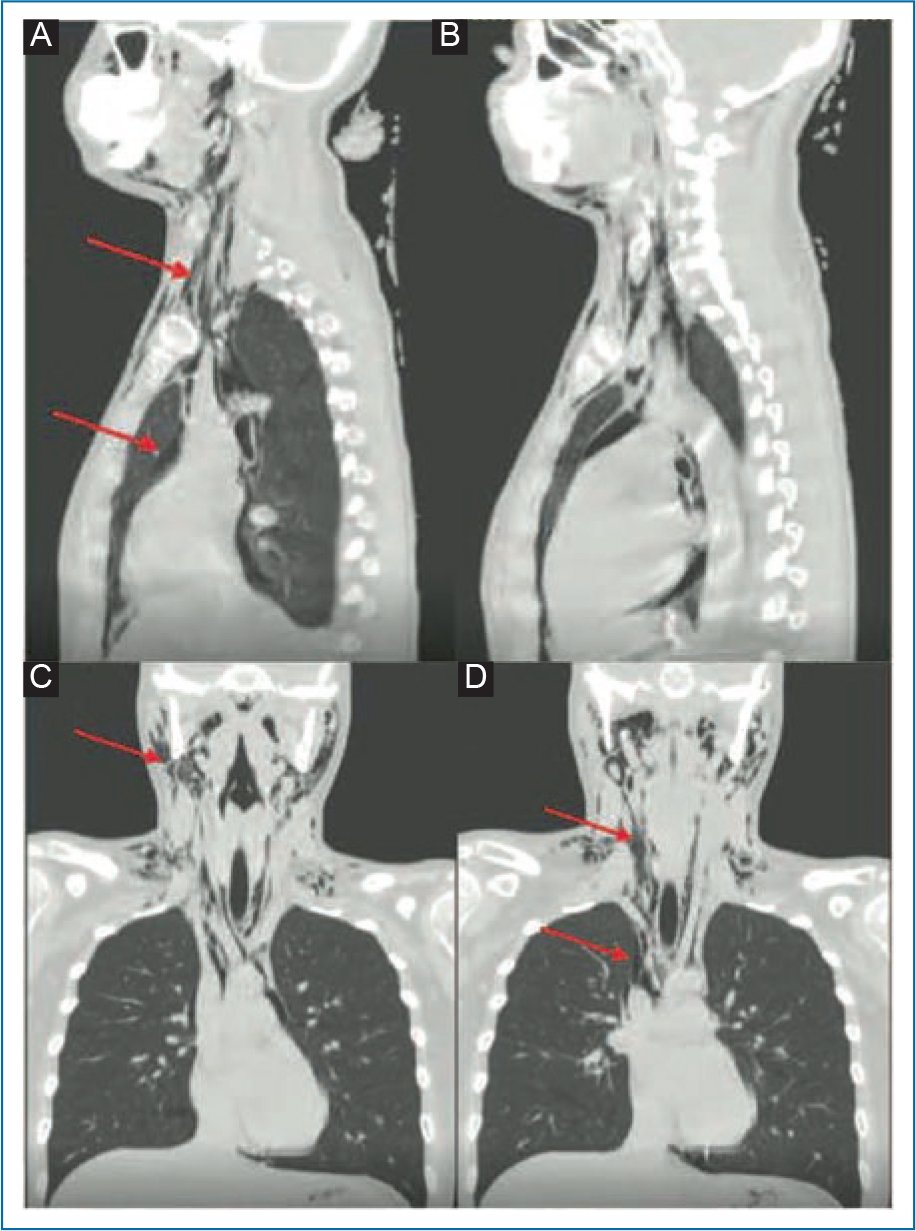
Figure 1. Chest computed tomography images. A and C: Initial images showing mediastinal and cervical emphysema (arrows). B and D: Images obtained 3 days after treatment demonstrating reduction of emphysema (arrows).
The condition was interpreted as secondary to a sudden increase in intrathoracic pressure, likely related to intense pushing maneuvers and fundal pressure during the expulsive phase (Kristeller maneuver). Esophageal perforation was ruled out by contrast esophagography, with no evidence of leak or disruption.
Conservative management was initiated with supplemental oxygen via nasal cannula and continuous clinical monitoring. Over the next 72 hours, the patient remained stable and asymptomatic, without dyspnea, chest pain, or signs of respiratory or hemodynamic compromise. Follow-up CT demonstrated significant reduction of mediastinal and subcutaneous emphysema, and the patient was discharged in good general condition (Fig. 2).
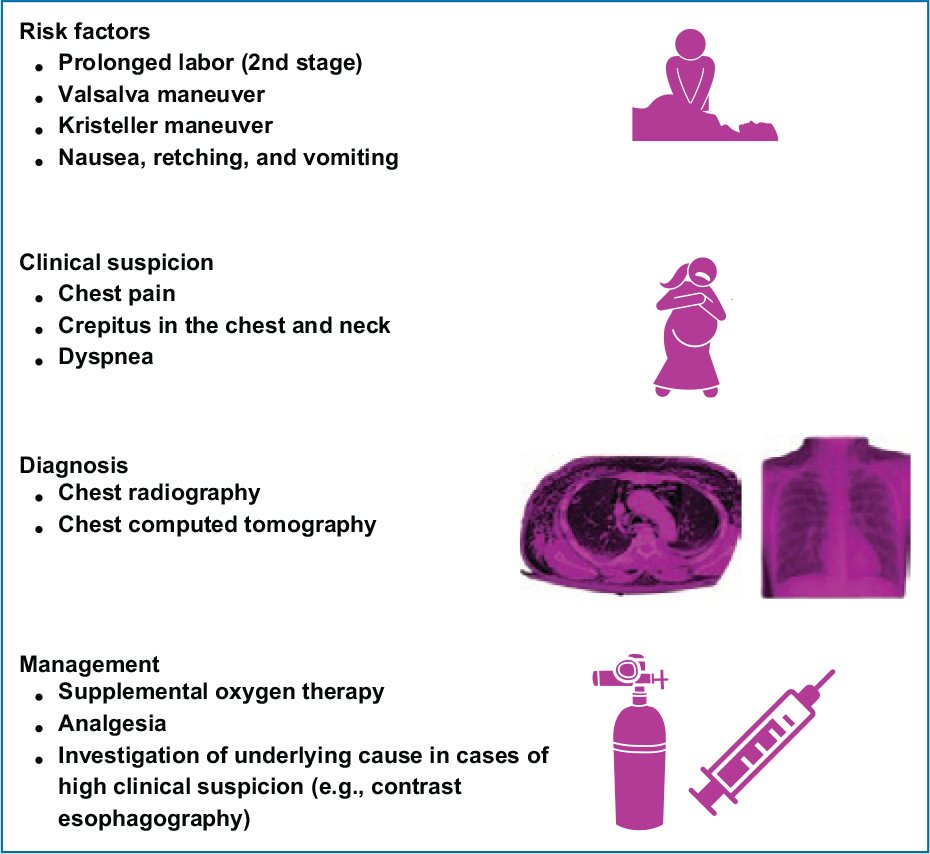
Figure 2. Approach to subcutaneous emphysema and pneumomediastinum in the peripartum period.
Discussion
We present the case of a postpartum patient diagnosed with pneumomediastinum and subcutaneous emphysema. Although uncommon, these conditions are typically associated with prolonged labor, particularly during the expulsive phase. Factors such as the Valsalva maneuver, coughing, vomiting, and intense physical effort may increase intrathoracic pressure and precipitate these complications1,2.
In this case, the patient was instructed to push while pulling on a sheet held distally by a medical intern, increasing effort. Her legs were flexed for approximately 1 hour. The Kristeller maneuver was also performed. Both interventions increase positive intrathoracic pressure and may trigger pneumomediastinum and subcutaneous emphysema3. Similar cases have been reported in patients undergoing such maneuvers during labor4,5.
From a pathophysiologic standpoint, spontaneous pneumomediastinum is most widely caused by the Macklin effect, which involves rupture of peripheral alveoli due to a sudden increase in intra-alveolar pressure. Air dissects along peribronchial and perivascular sheaths toward the mediastinum without direct injury6. This mechanism is the most frequent cause in young patients without underlying pulmonary disease. Sustained expulsive effort during labor may exacerbate this phenomenon7.
In more severe cases, airway rupture (trachea or main bronchi) may occur, although rare in obstetric settings. In the presence of suggestive symptoms such as severe odynophagia, intense chest pain, dyspnea, fever, or clinical signs of mediastinitis, esophageal perforation should be considered, and contrast esophagography with water-soluble contrast is indicated7,8. However, due to its low incidence rate, this is not recommended routinely. In this case, chest CT showed no evidence of esophageal or airway injury.
Treatment depends on clinical severity. In most cases, management is conservative and includes rest, supplemental oxygen (to promote mediastinal air reabsorption), analgesia if needed, and close clinical observation9,10. In patients with respiratory compromise, associated pneumothorax, or signs of mediastinal tension, invasive intervention such as mediastinal drainage or thoracotomy may be required.
Our patient was treated with low-flow oxygen via nasal cannula, with good tolerance and progressive improvement. Hospital observation lasted 72 hours, including continuous vital sign monitoring, respiratory evaluation, and follow-up CT documenting significant reduction of mediastinal and subcutaneous emphysema. As she remained asymptomatic without clinical deterioration, she was discharged without complications.
Although spontaneous pneumomediastinum in the obstetric setting is rare, early recognition, targeted clinical management, and appropriate follow-up allow favorable outcomes in most cases.
Conclusions
Pneumomediastinum and subcutaneous emphysema during the peripartum period are rare and usually nonsevere conditions managed with supplemental oxygen, analgesics, and observation. They should be considered in the presence of risk factors such as prolonged labor, arching, vomiting, or situations that increase positive intrathoracic pressure, including the Kristeller maneuver.
Funding
The authors declare that no funding was received.
Conflicts of interest
The authors declare no conflicts of interest.
Ethical considerations
Protection of humans and animals. The authors declare that no experiments were performed on humans or animals for this research.
Confidentiality, informed consent, and ethical approval. The authors followed institutional confidentiality protocols, obtained informed consent from the patient, and received Ethics Committee approval. The recommendations of the SAGER guidelines were followed according to the nature of the study.
Statement on artificial intelligence use. The authors declare that no generative artificial intelligence tools were used in the preparation of this manuscript.
\