Introduction
Anatomic variants of the tracheobronchial tree are uncommon, occurring in approximately 1% to 12% of the general population1. Bronchial isomerism refers to a disorder of bronchopulmonary laterality. Left bronchial isomerism is characterized by bilateral bilobed lungs, whereas right bronchial isomerism is characterized by bilateral trilobed lungs2. Bronchial isomerism is often asymptomatic; however, it may manifest with recurrent cough, hemoptysis, or respiratory infections3,4.
Pulmonary laterality disorders have also been associated with an increased risk of malignancy. Cases of pulmonary situs inversus associated with gastric, rectal, and pancreatic cancer have been reported5.
Pulmonary tissue contains neuroendocrine cells located within the bronchial epithelium. These cells may undergo hyperplasia as part of a chronic inflammatory response. When DIPNECH extends beyond the bronchial epithelial basement membrane, the term tumorlet is used. Tumorlet is a descriptive rather than a strictly histologic term, referring to a neuroendocrine proliferation measuring less than 0.5 cm6. Tumorlets are generally benign and are usually diagnosed incidentally, representing a pathologic finding without clear clinical significance. Associations with several neoplasms, including breast cancer, lung cancer, and thoracic lymphomas, have been described.
We report the case of a patient with recurrent respiratory infections leading to left lower lobe bronchiectasis associated with a right bronchial isomerism variant. Histopathologic examination of the resected tissue revealed an incidental tumorlet.
Case presentation
A 44-year-old woman with a past medical history of bronchiectasis and recurrent pneumonias presented with superinfection of bronchiectasis caused by resistant Pseudomonas aeruginosa. Chest computed tomography (CT) (Figure 1A) demonstrated abnormal bronchial branching suggestive of an accessory pulmonary lobe. However, bronchial reconstruction imaging revealed three left pulmonary lobes (Figure 1B), with the lower bronchus accompanied by a lobar artery (Figure 1C). Pulmonary function tests showed a forced expiratory volume in 1 second (FEV1) of 0.9 L, forced vital capacity (FVC) of 2.14 L, FEV1/FVC ratio of 42%, and diffusion capacity for carbon monoxide (DLCO) of 18.1 mL/min/mm Hg.
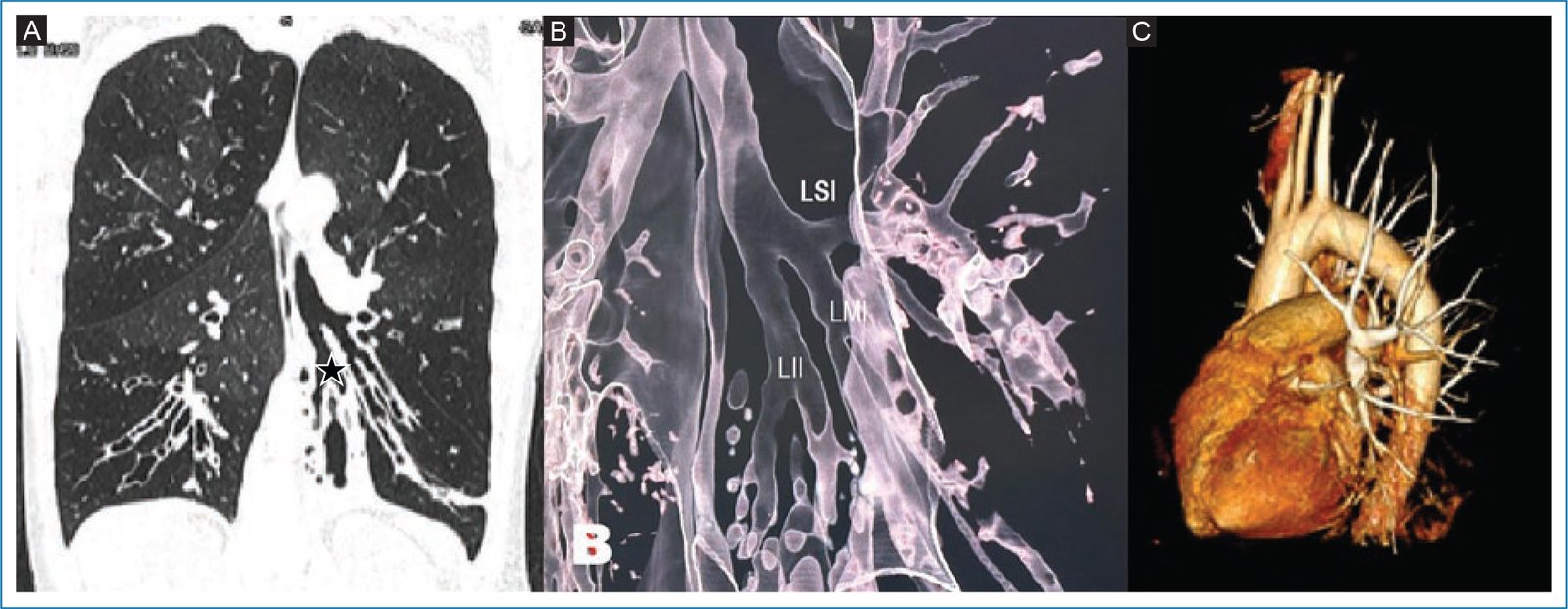
Figure 1. A: chest computed tomography (CT), lung window, coronal section at the level of the left main bronchus. Beaded bronchiectasis (asterisk) and division into 3 bronchi (upper, middle, and lower) are observed. B: 3D reconstruction demonstrating a secondary carina with division into 3 lobar bronchi. C: vascular reconstruction of the arterial pattern showing arterial supply to the left upper, middle, and lower lobes.
Given borderline pulmonary function, the patient was scheduled for left lower lobe segmentectomy. Intraoperatively, the left lung was found to have three lobes: superior, middle, and inferior (Figure 2A). A left lower lobectomy was performed with individual hilar vascular and bronchial control (Figure 2B). A 24-Fr pleural drain was placed.
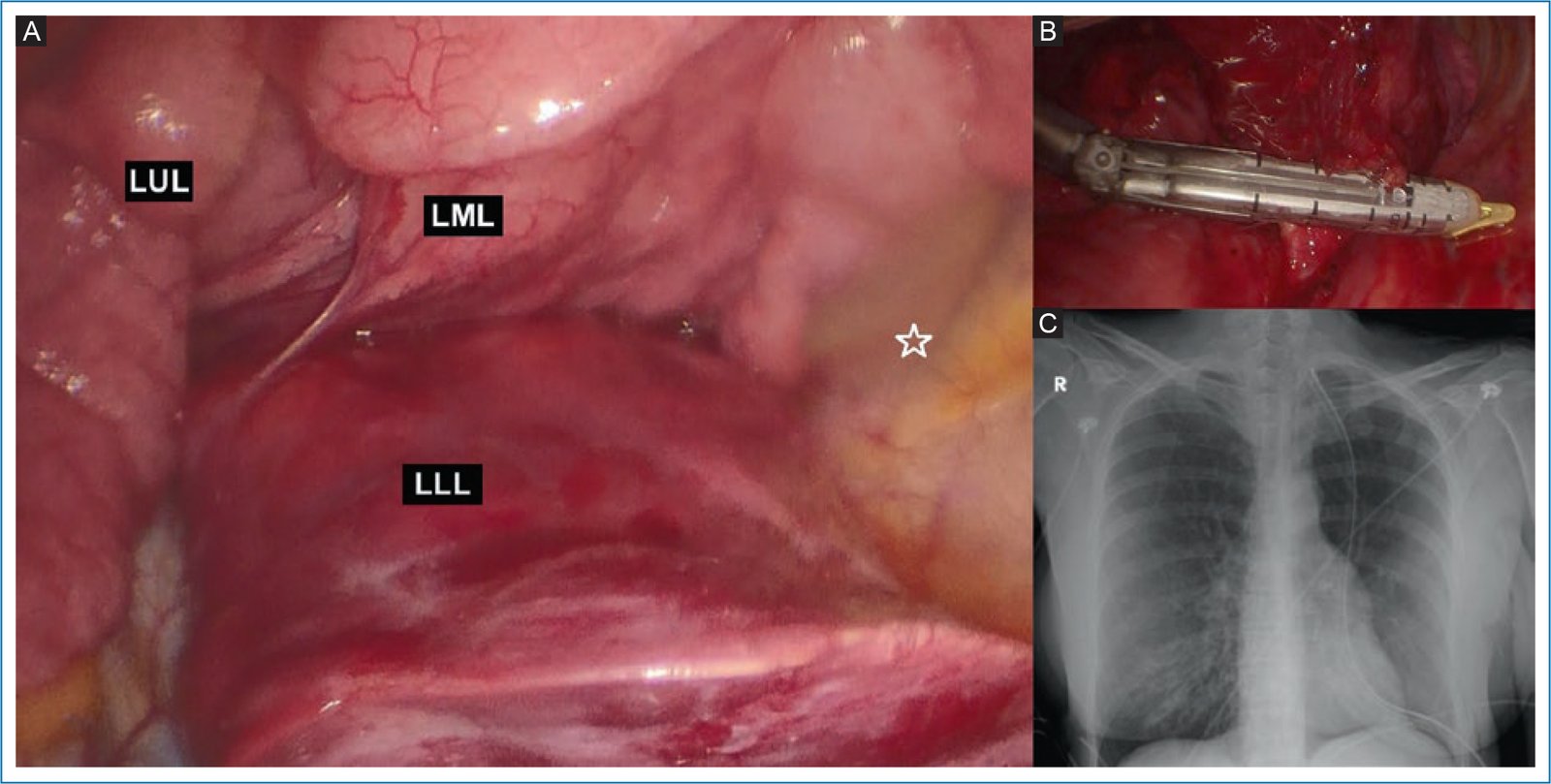
Figure 2. A: intraoperative photograph demonstrating major and minor fissures dividing the left lung into the left upper lobe (LUL), left middle lobe (LML), and left lower lobe (LLL). The asterisk marks the posterior wall of the left hemithorax. B: vascular control of the left lower lobe artery. C: postoperative posteroanterior chest radiograph showing adequate pulmonary expansion.
The patient had an uneventful postoperative course, with chest tube removal on postoperative day 3 (Figure 2C) and hospital discharge on day 5.
Histopathologic examination revealed chronic bronchiectasis and a 3-mm tumorlet composed of nests of cells with moderate cytoplasm and nuclei displaying “salt-and-pepper” chromatin. Immunohistochemistry was positive for synaptophysin and chromogranin.
Following isolation of Pseudomonas aeruginosa, the patient completed a 14-day course of ceftazidime, followed by 14 days of outpatient amikacin therapy.
Discussion
The tracheobronchial tree is a branching system that conducts air from the trachea to the acini. Various anatomic variants have been described, including tracheal bronchus, accessory cardiac bronchus, tracheal diverticula, bridging bronchus, and tracheobronchial isomerism. Although uncommon, these anomalies are typically asymptomatic. In symptomatic patients, signs may include cough, hemoptysis, and recurrent respiratory infections1.
Bronchial isomerism is a disorder of pulmonary laterality and has been associated with mutations in the ZIC3 gene, a zinc-finger transcription factor involved in establishing left–right symmetry during embryonic lung development.
Bronchial isomerism was first described by Bush in 1999. Left bronchial isomerism is characterized by bilateral bilobed lungs, whereas right bronchial isomerism is characterized by bilateral trilobed lungs. Clinical sigs are generally related to associated anomalies. In the present case, the left isomeric inferior lobe demonstrated abnormal bronchial morphology characterized by bronchiectasis, leading to recurrent infections with isolation of antimicrobial-resistant microorganisms, a situation that ultimately prompted surgical management.
Pulmonary tissue contains neuroendocrine cells located within the bronchial and bronchiolar epithelium. DIPNECH is a rare entity associated with constrictive bronchiolitis and was first described by Aguayo in 1992. DIPNECH may occur as part of an inflammatory response and typically remains confined to the bronchial epithelial basement membrane. In patients with carcinoid tumors, DIPNECH has been considered a preneoplastic lesion. Approximately 47.4% of patients with DIPNECH develop typical carcinoid tumors, whereas 15.8% develop atypical carcinoids. When diffuse neuroendocrine cell hyperplasia extends beyond the basement membrane and measures < 5 mm, it is termed a tumorlet; lesions > 5 mm are classified as carcinoid tumors7,8. Histologically, tumorlets demonstrate argyrophilic staining properties and are positive for synaptophysin and chromogranin on immunohistochemistry. The cells typically exhibit regular, round to oval or spindle-shaped nuclei with finely dispersed (“salt-and-pepper”) chromatin.
On high-resolution computed tomography (CT), DIPNECH is characterized by mosaic attenuation due to air trapping, bronchial wall thickening, and bronchiectasis. Nodular thickening of the bronchial wall represents the most direct radiopathologic correlate of submucosal neuroendocrine cell proliferation9.
Five-year survival for DIPNECH is approximately 83% vs 93% for typical carcinoid tumors and 69% for atypical carcinoids. According to the most recent World Health Organization classification, DIPNECH is considered a preinvasive lesion within the spectrum of pulmonary neuroendocrine proliferations, followed by tumorlets and carcinoid tumors. In this context, the European Society for Medical Oncology recommends lifelong surveillance, given the risk of recurrence associated with carcinoid tumors10.
Conclusions
We report the case of a female patient with bronchiectasis-related infection associated with a pulmonary laterality anomaly. Histopathologic examination incidentally revealed a tumorlet. Although the literature consists primarily of case reports, this entity should be considered in patients with tracheobronchial morphologic variants and potential neoplastic risk.
Funding
This study did not receive specific funding from public sector agencies, commercial entities, or nonprofit organizations.
Conflicts of interests
The authors declared no conflicts of interest whatsoever.
Ethical considerations
Protection of human and animal subjects. The authors declare that no experiments involving human participants or animals were performed for this study.
Confidentiality, informed consent, and ethical approval. The authors adhered to their institution’s protocols regarding patient confidentiality and obtained informed consent from the patients. Approval from the institutional ethics committee was obtained, as applicable. The recommendations of the SAGER guidelines were followed according to the nature of the study.
Declaration on the use of artificial intelligence. The authors declare that no generative artificial intelligence tools were used in the drafting of this manuscript.
