Introduction
Destroyed lung (destruens lung) is a rare complication of several disease entities, most frequently secondary to Mycobacterium tuberculosis infection, which accounts for approximately 80% of cases. It typically occurs in patients with delayed diagnosis and treatment. The imaging findings reflect compensatory changes in the remaining pulmonary parenchyma. Despite adequate antituberculous therapy, complications following destruction of the affected lung are diverse and may be fatal, particularly in the presence of hemoptysis. Additionally, patients experience impaired quality of life due to increased susceptibility to opportunistic infections. We report a case of destroyed lung due to M. tuberculosis infection, diagnosed in the context of a major hemoptysis episode.
Case presentation
A 27-year-old woman from Tepatitlán, Jalisco, Mexico, homemaker, single, from a low socioeconomic background, with a maternal family history of breast cancer, presented for evaluation. She had no relevant environmental exposures. She reported contact with a chronic cougher (father), although the cause was unknown. Since childhood, she had experienced chronic cough and had been treated since 2007 as having asthma without spirometric confirmation, using short-acting bronchodilators as needed. In October 2019, she sought medical attention for weight loss and productive cough. Chest radiography revealed a cavitary lesion in the left pulmonary apex. Serial sputum acid-fast bacilli smears were positive. She was diagnosed with cavitary pulmonary tuberculosis and received isoniazid, rifampin, pyrazinamide, and ethambutol for 60 doses, followed by rifampin and isoniazid for 45 doses. Sputum cultures at the end of therapy were negative, and she was declared cured in April 2020.
The patient continued to have a nonproductive cough after completing antituberculous therapy. In March 2023, she developed low-grade fever, followed in April 2023 by hemoptysis quantified at approximately 500 mL. On physical examination, she was underweight. The chest was asymmetric, with absent vocal fremitus and hyperresonance over the left hemithorax, and decreased breath sounds consistent with a rarefaction syndrome. Laboratory testing showed hemoglobin 9 g/dL, hematocrit 28%, platelets 202 × 103/µL, leukocytes 6.72 × 103/µL, neutrophils 58%, and glucose 102 mg/dL. Chest computed tomography (CT) in lung window demonstrated anterior herniation of the right lung, mediastinal traction toward the left, narrowing of the intercostal spaces, and areas of decreased attenuation following bronchial pathways suggestive of cystic bronchiectasis (Figure 1).
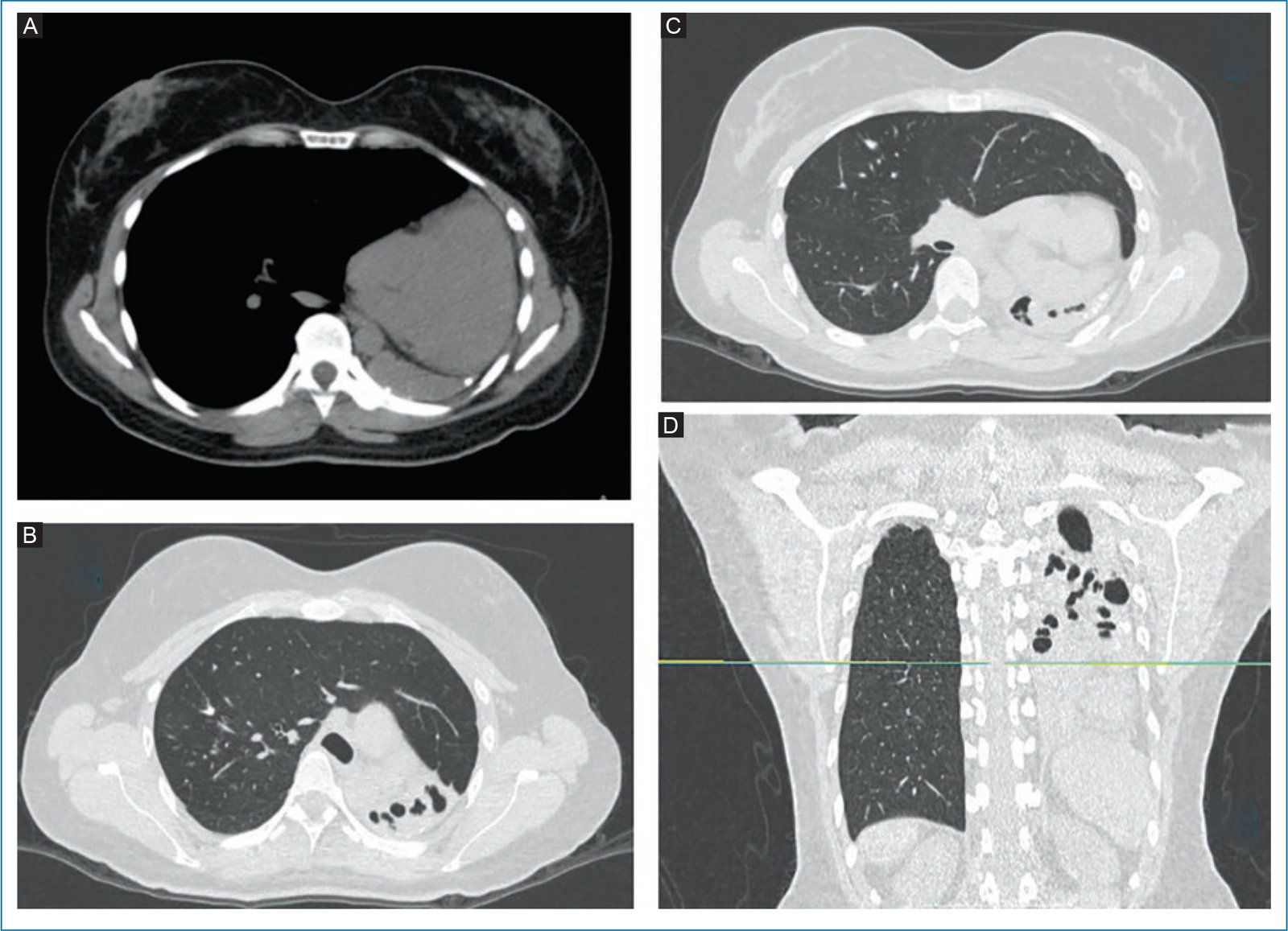
Figure 1. A: axial chest CT in mediastinal window showing mediastinal shift to the left and rib crowding. B y C: axial lung window CT images demonstrating pulmonary parenchymal herniation and mediastinal displacement with areas of increased attenuation containing regions of decreased attenuation suggestive of bronchiectasis. D: coronal lung window image showing absence of pulmonary parenchyma in the left hemithorax, elevation of the ipsilateral hemidiaphragm, and cystic and varicose bronchiectasis.
Bronchoscopy revealed concentric narrowing of the middle third of the left main bronchus, preventing passage of the bronchoscope, suggestive of extrinsic compression vs external scarring without evidence of endobronchial infiltration. Bronchoalveolar lavage RT-PCR for tuberculosis and mycobacterial culture were negative. Fungal culture yielded Aspergillus nidulans (Figure 2). The patient received itraconazole 200 mg twice daily with favorable clinical response. Due to the risk of recurrent bleeding and bronchiectasis colonization, she was evaluated by thoracic surgery and considered a candidate for left pneumonectomy, pending pulmonary function assessment and nutritional optimization.
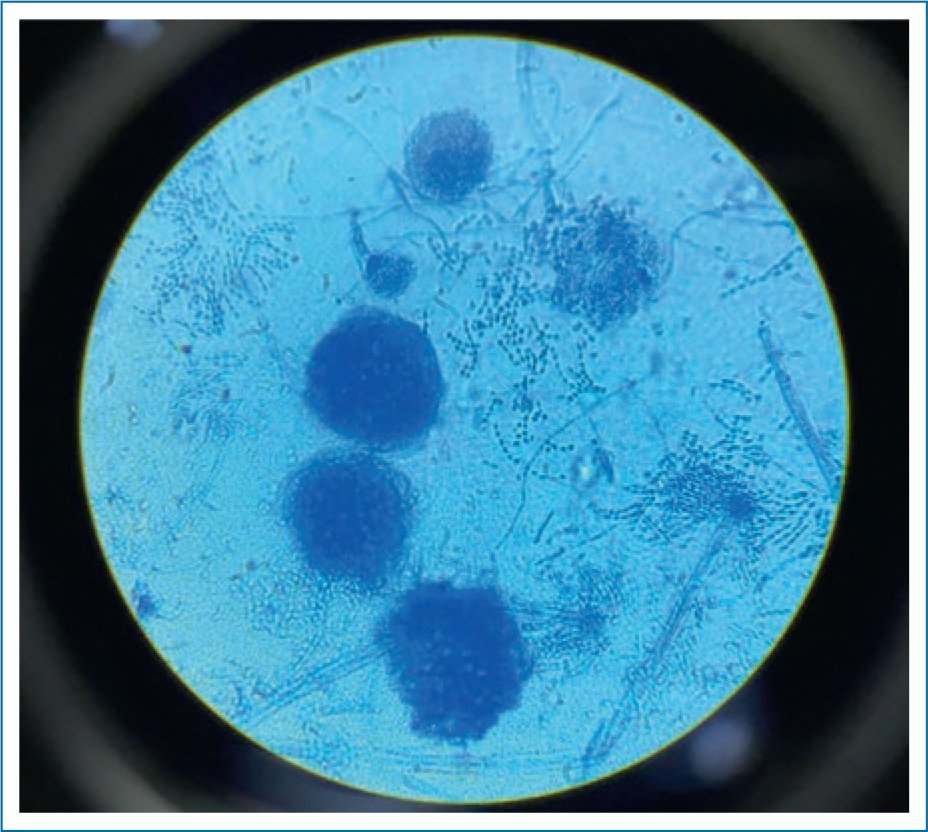
Figure 2. Isolation of Aspergillus nidulans with Hülle cells on lactophenol cotton blue stain.
Discussion
Tuberculosis is an infectious disease caused by Mycobacterium tuberculosis. This pathogen produces a broad spectrum of disease involving both pulmonary and extrapulmonary sites1. According to the 2021 World Health Organization (WHO) report, approximately 25% of the global population has immunologic evidence of prior infection with M. tuberculosis. In Mexico, according to the 2022 national tuberculosis surveillance report, 78.7% of cases involved pulmonary disease, followed by miliary tuberculosis (4.7%) and lymph node involvement (4.6%). Mortality data indicate that up to 1.4 million deaths were attributed to this pathogen in 2020, making it the 2nd leading infectious cause of death worldwide that year, after severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)2.
The clinical spectrum of tuberculosis depends largely on host susceptibility, with increased risk observed in individuals with diabetes mellitus, alcohol use disorder, or HIV infection. Pulmonary tuberculosis is classically categorized into 3 forms3 (Table 1).
Table 1. Pathologic forms of pulmonary infection due to Mycobacterium tuberculosis and their imaging signs
| Primary | Consolidation, predominantly in the upper lobes; pleural effusion; miliary pattern; hilar and mediastinal lymphadenopathy |
| Postprimary (reactivation) | Cavitary and/or nodular disease |
| Latent | Positive tuberculin skin test or molecular testing without imaging or clinical findings suggestive of primary or postprimary tuberculosis |
In recent years, the concept of post-tuberculosis disease has gained increasing attention because of the long-term sequelae that may persist despite appropriate antimicrobial treatment. Post-tuberculosis disease is defined as chronic respiratory abnormalities, with or without associated symptoms, attributable to prior pulmonary tuberculosis. Its reported prevalence varies widely, ranging from 18% to 87%, reflecting the lack of standardized definitions and limited epidemiologic data1. Destroyed lung (pulmón destruido) is included within this spectrum of post-tuberculosis sequelae.
Destroyed lung is defined as a combination of parenchymal and pleural destruction manifested radiologically by cavitation, bronchiectasis, loss of lung volume, and mediastinal shift toward the affected side5. It is more frequently reported in countries with limited health care resources. The principal cause is M. tuberculosis infection (approximately 80% of cases), followed by necrotizing pneumonia and advanced stages of bronchiectasis6. This complication develops in approximately 1.3% of patients despite appropriate antituberculous treatment7.
Risk factors identified in case series include male sex, a mean age at presentation of approximately 55 years, and a history of tuberculosis diagnosed during childhood or adolescence5. Patients are often initially asymptomatic and later develop chronic symptoms, including productive cough (occasionally purulent), hemoptysis, fever, and dyspnea. Physical examination may reveal thoracic asymmetry on the affected side, with decreased and horizontally oriented intercostal spaces8. On posteroanterior chest radiography, findings may include diffuse opacification of the affected hemithorax, ipsilateral mediastinal deviation, cystic bronchiectasis, and cavitation. On lateral projection, retrosternal hyperlucency may be observed, consistent with compensatory hyperinflation of the contralateral lung9.
Computed tomography findings described by Shital et al are summarized in figure 310. Case series have reported left lung predominance in approximately 58.1% of cases. Anterior herniation of the contralateral lung into the mediastinum, involving the upper and middle lobes, occurs in 92% of cases; posterior herniation involving the lower lobe occurs in 85%; and simultaneous anterior and posterior herniation occurs in 77%5,11. The higher frequency of left-sided involvement is attributed to bronchial anatomy, as the left main bronchus is longer, narrower, and more horizontally oriented than the right, which impairs secretion drainage12.
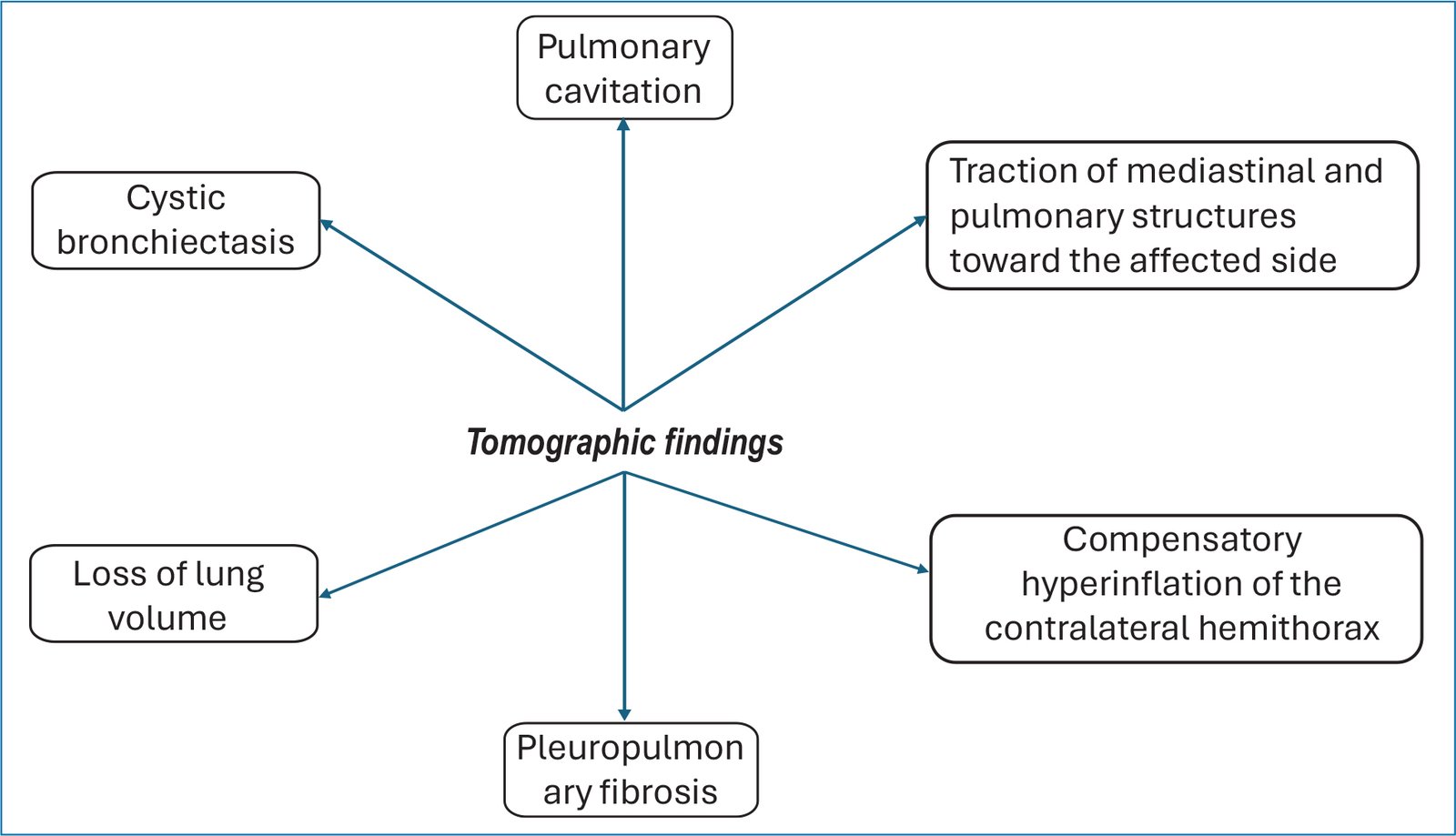
Figure 3. Tomographic findings of destroyed lung.
Surgical management is reserved for patients with complications such as massive hemoptysis, bronchopleural fistula, or empyema. Described procedures include pneumonectomy, pleuropneumonectomy, and bronchopleural fistula repair combined with pneumonectomy. The specific indication for each procedure remains controversial, and no clear consensus exists. In a case series of 172 patients, pleuropneumonectomy was performed in those with destroyed lung and pleural adhesions; pneumonectomy was preferred in the absence of empyema or bronchopleural fistula; and combined bronchopleural fistula repair with pneumonectomy was selected when fistula was present13. The overall operative mortality for pneumonectomy has been reported at approximately 4%. The most common postoperative complications include bronchopleural fistula (12%) and empyema (32%). Absolute contraindications include forced expiratory volume in 1 second (FEV1) < 2 L and diffusion capacity of the lung for carbon monoxide < 60% predicted.
Coinfection has been described in small case series in up to 46.1% of patients, most commonly involving gramnegative organisms such as Pseudomonas aeruginosa and Haemophilus influenzae, and less frequently fungal infections14.
Conclusions
Destroyed lung is a rare but severe complication of M. tuberculosis infection. Although early and appropriate antituberculous therapy reduces its incidence, characteristic imaging findings allow diagnosis when it occurs. Management recommendations continue to evolve.
Funding
This study received no specific funding from public, commercial, or nonprofit agencies.
Conflicts of interests
The authors declared no conflicts of interest whatsoever.
Ethical considerations
Protection of humans and animals. No experiments were performed in humans or animals.
Confidentiality and informed consent. The study does not involve identifiable patient data and did not require ethics committee approval. SAGER guidelines: Not applicable.
Declaration on the use of artificial intelligence. The authors declare that no generative artificial intelligence was used in the preparation of this manuscript.
