Brief descriptive epidemiology
Coronavirus disease 2019 (COVID-19) is a respiratory infection caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), first identified in December 2019 in Wuhan, China. Since then, it has spread to all continents and caused multiple epidemic waves. As of May 2024, more than 775 million confirmed cases and over 7 million deaths have been reported worldwide1. In Mexico, as of June 25, 2023, more than 7.6 million cumulative cases and over 334,000 deaths have been reported since the beginning of the pandemic2, with a case fatality rate of 4.39% vs the global rate of 0.9%. This difference in case fatality between Mexico and the global estimate is likely due to underestimation of the true burden of disease in Mexico, as only a fraction of cases are diagnosed and reported. Although official figures provide an approximation of disease burden, substantial underestimation is acknowledged, particularly during waves with higher transmission, when confirmatory testing rates were lower. The reported global case fatality rate has progressively declined since the beginning of the pandemic, attributable to both acquired immunity (from infection or vaccination) and the availability of more effective treatments and better-adapted health systems3. International epidemiologic surveillance has documented wide regional and national variation in the distribution of cases, hospitalizations, and deaths, influenced by unequal access to vaccines, health services, mitigation measures, and the prevalence of comorbidities in the population4.
Before the World Health Organization (WHO) declared the end of the global public health emergency for COVID-19 in May 2023, SARS-CoV-2 infection was estimated to have caused approximately 15 million excess deaths in 2020 and 2021 alone. As SARS-CoV-2 becomes endemic, it remains an important cause of disease worldwide5.
Transmission dynamics and viral shedding
The primary route of transmission of SARS-CoV-2 is direct airborne spread through close person-to-person contact at short distance (approximately 2 meters). Virus released in respiratory secretions when an infected person speaks, coughs, sneezes, or sings may infect another person if inhaled or if it comes into direct contact with mucous membranes. Infection may also occur if contaminated hands touch the eyes, nose, or mouth after contact with respiratory secretions or contaminated surfaces; however, surface transmission is considered unlikely to be a major route6. Moreover, SARS-CoV-2 has been detected in nonrespiratory samples, including stool, blood, ocular secretions, and semen; however, based on current evidence, transmission through these sites is unlikely7. Respiratory droplets expelled when an infected individual speaks, coughs, or sneezes typically measure 5-10 μm in diameter. In contrast, aerosols are droplet nuclei formed after evaporation and are generally < 5 μm in size8. Respiratory droplets and aerosols expelled during sneezing or coughing may travel distances of 3.6 to 7.9 meters9–significantly farther than the 2-meter social distancing guideline recommended by the US Centers for Disease Control and Prevention (CDC). Due to their small size and minimal gravitational influence, aerosols may remain suspended in the air for prolonged periods, posing an additional risk of airborne transmission, particularly in poorly ventilated indoor environments.
Viral particles in exhaled droplets and aerosols may bind to atmospheric PM2.5 particles; however, the contribution of this pathway to pandemic transmission remains uncertain10. Transmission may also occur during aerosol-generating medical procedures, including nasopharyngeal sampling, orotracheal intubation, invasive and noninvasive ventilation, use of nebulizers, high-flow nasal oxygen, bronchoscopy, and related interventions.
Higher transmission rates occur with close contact and within households; however, in most cases (79%), the specific source of exposure remains unknown11. Peak transmissibility occurs approximately 5-8 hours before symptom onset and is highest during the early stages of illness, when viral RNA levels in upper respiratory tract samples are greatest12. Transmission beyond 7-10 days after symptom onset is unlikely, particularly in immunocompetent patients with non-severe infection. A contact-tracing study showed that individuals exposed to infected patients more than 6 days after symptom onset did not develop infection13.
The duration of viral shedding is variable and may increase with age and disease severity. A meta-analysis reported a median duration of viral RNA detection in respiratory samples of 18 days from symptom onset14. In some individuals, viral RNA was detectable in 5% of cases into the fifth week and, in rare cases, for several months15,16. However, detection of viral RNA does not necessarily indicate the presence of viable virus17.
Infectious virus has only been detected in respiratory samples with high viral RNA concentrations, which correspond to lower cycle threshold (Ct) values on reverse transcription-polymerase chain reaction (RT-PCR) testing. The Ct threshold for positive viral culture typically ranges from 24 to 3218,19. According to the US CDC, three days after clinical recovery, if viral RNA remains detectable in upper respiratory tract samples, RNA concentrations are generally below levels at which viable virus can be reliably isolated. Isolation of infectious virus from upper respiratory tract samples beyond 10 days after symptom onset is rare18,20.
Natural history of SARS-CoV-2 infection
The incubation period, defined as the time between exposure to the virus and the onset of COVID-19 symptoms, is approximately 5.2 days (95% CI, 4.1-6.4). In some cases, it may be as short as 36 hours or as long as 14 days. Presymptomatic and asymptomatic individuals can also transmit the disease. Presymptomatic individuals transmit the virus a few days before symptom onset, when viral load is highest, often without being aware that they are infecting others21. The risk of transmission during the presymptomatic phase is high and, according to some reports, contributed to 48% and 62% of transmissions in Singapore and China, respectively22. Although reported, the role of asymptomatic cases in transmission has been difficult to quantify23. It is reasonable to assume that in a significant proportion of secondary cases, transmission occurs before symptom onset and, in some cases, in the absence of symptoms.
The basic reproduction number (Ro) is a useful epidemiologic concept for studying disease transmission and is defined as the average number of new cases generated by each infected individual. Ro is an important public health measure in terms of disease spread and eventual containment. It is not a fixed value and depends on various factors, including population susceptibility, demographics, socioeconomic conditions, and seasonality. Typically, Ro is < 1 when the disease is under control and > 1 when it is spreading. During an outbreak, interventions aimed at controlling transmission are intended to reduce the Ro value24. The average Ro for COVID-19 has been estimated at 2.2 to 2.7, with a case doubling time of 6 to 7 days25. Because Ro represents a mean value, its interpretation may obscure a highly dispersed distribution in which a small number of infected individuals account for most secondary transmission. In COVID-19, it is estimated that approximately 10% of infected individuals are responsible for 80% of secondary infections26.
Understanding the risk of infection is essential for controlling viral spread. Transmission risk varies by setting and depends on duration of exposure, viral load, and physical space. Enclosed environments with poor ventilation, large crowds, and prolonged contact with an infected person substantially increase the likelihood of secondary infection. In many instances, a single infected individual has transmitted the virus to large numbers of people during events such as conferences, religious services, sporting events, or social gatherings. The longer a group remains together, the higher the probability of viral spread. Indoor, poorly ventilated spaces are particularly conducive to transmission. A study in Japan estimated that the likelihood of transmission in enclosed environments was 18.7 times higher than in outdoor settings27. In such environments, the effective reproduction number (Ro) may increase substantially, reaching values as high as 11 in certain closed workplace settings28,29. The Texas Medical Association developed a COVID-19 risk chart ranking activities from 1 to 10 according to exposure risk. Examples, ordered from lowest to highest risk, include: pumping gasoline (2), playing tennis (2), dining outdoors (4), going to the beach (5), visiting a shopping mall (5), swimming in a public pool (6), dining indoors (7), air travel (7), working out at a gym (8), and attending a concert or stadium event (9)30.
Course of the disease
Once clinical disease manifests, its progression over time is determined by 2 overlapping pathophysiologic mechanisms: one triggered by viral replication and the other by the host immune response. Siddiqi and Mehra proposed a three-stage classification system with three severity categories, each characterized by distinct clinical findings, treatment response, and outcomes. Stage I occurs during the early days of infection and is dominated by viral replication, with symptoms such as malaise, fever, and cough. The immune response is activated during this stage (Figure 1)31. Patients whose disease remains confined to this stage generally recover and have a favorable prognosis. Stage II is characterized by viral involvement of the pulmonary parenchyma, leading to pneumonia and an inflammatory response. The extent of pneumonia and the intensity of inflammation determine the degree of hypoxia. Stage III develops in a minority of patients and represents the most severe phase of the disease. It is marked by a hyper-inflammatory syndrome, manifested not only by severe hypoxia but also by extrapulmonary involvement31.
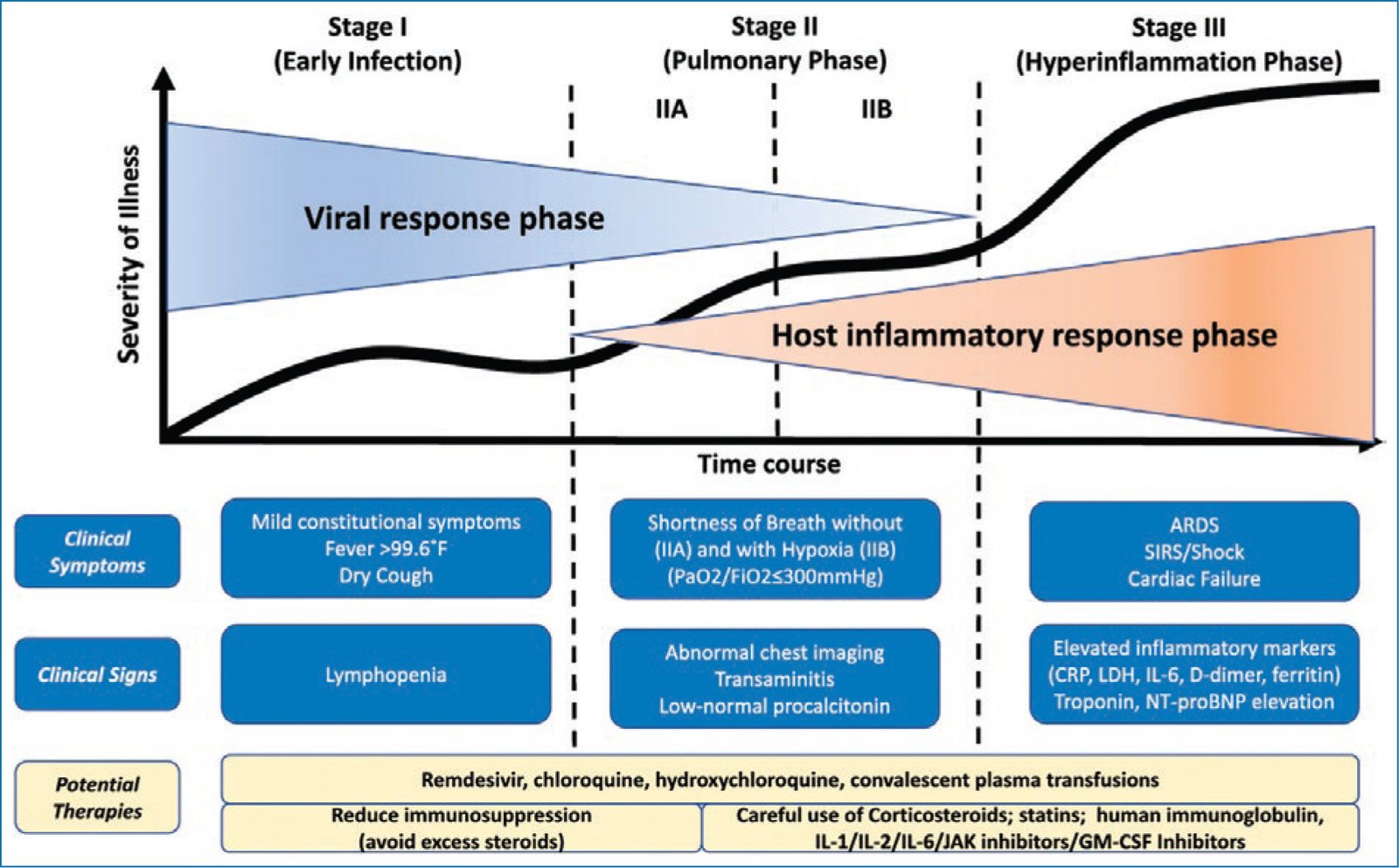
Figure 1. Classification of the stages of COVID-19 disease and potential therapeutic targets (taken and adapted from Siddiqi and Mehra.31). Licensed by Elsevier number 5101931362917, dated July 4, 2021.
The largest report of COVID-19 cases, including 72,314 patients, demonstrated that 81% developed mild disease and 5% developed severe disease characterized by respiratory failure, septic shock, and multiorgan dysfunction. Among severe cases, mortality reached 50%, particularly in patients > 50 years. The overall case fatality rate was 2.3%, increasing to 3.6% in individuals aged 60-69 years, 8.0% in those aged 70-79 years, and 14.8% in those > 80 years32,33.
Individuals of all ages are at risk for infection and severe disease. However, patients aged ≥ 60 years and those with underlying comorbidities–such as diabetes, obesity, chronic lung disease, chronic kidney disease, cardiovascular disease, cancer, and recipients of solid organ or hematopoietic stem cell transplantation–have a higher risk of severe COVID-19. An analysis by Stokes et al. of confirmed cases reported to the US CDC between January 22nd and May 30th, 2020, showed that hospitalization rates were 6 times higher in patients with preexisting medical conditions than in those without (45.4% vs 7.6%), and mortality was 12 times higher (19.5% vs 1.6%)34. Sex-related differences have also been observed, with men at higher risk of severe disease and mortality compared with women35.
Clinical signs range from asymptomatic infection to critical illness with respiratory failure, septic shock, and multiorgan failure. Most symptomatic patients present with a variable combination of fever, cough, dyspnea, sore throat, anosmia, dysgeusia, anorexia, nausea, malaise, myalgias, and diarrhea. Among 373,883 symptomatic confirmed cases in the United States, 70% reported fever, cough, and shortness of breath; 36% reported myalgias; and 34% reported headache34. In addition to respiratory signs and symptoms, COVID-19 may produce extrapulmonary signs involving the cardiovascular, neurologic, hematologic, renal, hepatobiliary, endocrine, and GI systems. A meta-analysis of 8,697 patients in China reported laboratory abnormalities including leukopenia (23.5%), lymphopenia (47.6%), abnormal liver function (26.4%), abnormal renal function (10.9%), elevated C-reactive protein (65.9%), elevated cardiac enzymes (49.4%), elevated D-dimer (20.4%), and elevated procalcitonin (16.7%)36. Common radiographic findings include bilateral multifocal opacities on chest radiographs and bilateral peripheral groundglass opacities, with or without consolidation, on chest computed tomography.
Based on disease severity, the National Institutes of Health (NIH) have published guidelines that classify COVID-19 into five distinct categories in which adults with SARS-CoV-2 infection can be grouped. This classification takes into consideration the severity of clinical symptoms, laboratory and radiographic abnormalities, hemodynamic stability, and organ function.
– Asymptomatic or presymptomatic infection: Positive SARS-CoV-2 test without clinical symptoms consistent with COVID-19.
– Mild illness: Symptoms such as fever, cough, sore throat, malaise, headache, myalgia, nausea, vomiting, diarrhea, anosmia, or dysgeusia, without dyspnea or abnormal chest imaging.
– Moderate illness: Clinical or radiologic evidence of lower respiratory tract disease with oxygen saturation (SpO2) ≥ 94% on room air.
– Severe illness: SpO2 ≤ 94% on room air; PaO2/FiO2 < 300; respiratory rate > 30 breaths/min; lung infiltrates > 50% on imaging; or neutrophilia.
– Critical illness: Acute respiratory failure, septic shock, and/or multiorgan dysfunction. Patients with severe disease may develop acute respiratory distress syndrome (ARDS), typically approximately 1 week after symptom onset.
Prevention
Prevention of SARS-CoV-2 infection has evolved substantially since the beginning of the COVID-19 pandemic, adapting to vaccine availability, emerging scientific evidence, and the transmission dynamics of new variants. Current preventive strategies include both pharmacologic interventions (vaccination) and nonpharmacologic measures (mask use, ventilation, hygiene, diagnostic testing, isolation, and discontinuation of quarantine).
Vaccination remains the primary tool for preventing COVID-19 at both the individual and community levels. Multiple studies have demonstrated that immunization reduces the risk of symptomatic infection, hospitalization, and death38,39. Although effectiveness against infection may decline with the emergence of new variants, protection against severe disease and fatal outcomes remains substantial40.
The US Centers for Disease Control and Prevention (CDC) and the World Health Organization (WHO) recommend periodic booster doses, particularly for adults aged ≥ 60 years, immunocompromised individuals, pregnant women, and health care personnel, prioritizing updated formulations targeting circulating variants41,42.
Among nonpharmacologic measures, mask use was one of the earliest control interventions and continues to be effective, particularly in settings of high community transmission and in enclosed spaces with poor ventilation. High-efficiency respirators (N95, KN95, or equivalent) provide greater protection than surgical or cloth masks43.
Improving indoor ventilation is another key non-pharmacologic measure, as it reduces the concentration of viral particles in the air and lowers transmission risk. Recommended strategies include increasing natural ventilation by opening windows and using high-efficiency particulate air (HEPA) filtration systems in crowded indoor environments44. Basic hygiene measures – such as covering the mouth and nose when coughing or sneezing, frequent handwashing with soap and water, and use of alcohol-based hand sanitizers – remain essential to limit the spread of SARS-CoV-2 and other respiratory viruses45.
The availability of rapid antigen and molecular tests has facilitated early case identification. Symptom monitoring and timely testing in individuals with suspected exposure or compatible symptoms allow for prompt isolation and reduction of transmission risk46.
In March 2024, the CDC updated its guidance regarding isolation for individuals with confirmed SARS-CoV-2 infection. Unlike earlier recommendations that established a fixed 5-day isolation period followed by 5 additional days of mask use47,48, the updated guidance is based on clinical status. Symptomatic individuals are advised to remain in isolation until 2 criteria are met: (1) at least 24 hours have passed without fever in the absence of antipyretics, and (2) overall symptom improvement49. Once these criteria are satisfied, home isolation may be discontinued regardless of the total number of days since symptom onset. The CDC recommends maintaining additional precautions for the subsequent 5 days, including high-efficiency mask use, avoiding contact with vulnerable individuals, ensuring adequate ventilation, and reinforcing hygiene practices.
Quarantine – defined as restriction of activities in asymptomatic individuals exposed to a confirmed case – was widely implemented in 2020 and 2021, initially for up to 14 days and later reduced to 7 days with a negative test. In August 2022, the CDC eliminated quarantine recommendations for exposed individuals, replacing them with symptom monitoring for 10 days, mask use, and testing around day 5 after exposure. With the March 2024 update, the CDC confirmed that quarantine is no longer recommended. The current strategy emphasizes active clinical observation and protective measures, with isolation only if symptoms develop or a positive test result is obtained50,51.
In conclusion, preventive strategies for SARS-CoV-2 have shifted from rigid models to dynamic approaches adapted to the evolving epidemiologic context. Vaccination remains the cornerstone of prevention, complemented by nonpharmacologic interventions such as mask use in high-risk settings, ventilation, and hygiene. Isolation continues to be necessary in confirmed cases but is based on clinical criteria rather than fixed time intervals, while quarantine is no longer recommended for asymptomatic exposed individuals.
Future projection of the pandemic
Although the WHO declared the end of the global public health emergency for COVID-19 in May 2023, SARS-CoV-2 continues to circulate globally as a significant respiratory pathogen. In the foreseeable future, COVID-19 is expected to transition to an endemic pattern, characterized by seasonal circulation and sporadic surges associated with new variants or waning population immunity52.
Vaccines and antiviral therapies have substantially reduced disease severity, hospitalizations, and mortality. Nevertheless, prevention will continue to depend in part on nonpharmacologic interventions, particularly among vulnerable populations and during transmission peaks. Complete viral elimination appears unlikely in the short term due to high transmissibility, incomplete and transient immunity, and the ongoing emergence of variants with partial immune escape53.
Since its emergence, SARS-CoV-2 has generated multiple variants, some classified as variants of concern (VOCs) because of increased transmissibility or immune evasion. To date, the principal VOCs have included Alpha, Beta, Gamma, Delta, and Omicron, with Omicron predominating since late 2021. Within the Omicron lineage, subvariants such as XBB.1.5 and JN.1 have dominated at different times since 2023, demonstrating greater transmissibility but lower lethality compared with earlier variants.
Although current vaccines provide strong protection against severe disease and death, effectiveness against infection wanes over time and with the emergence of new variants. Herd immunity has not been achieved and is unlikely in the medium term because of heterogeneous vaccine coverage, ongoing viral evolution, and partial immunity from prior infections53.
Five-year projections suggest that COVID-19 incidence rate will depend on population immunity levels, duration of postinfection or postvaccination immunity, and the emergence of new variants. Additional factors include seasonality, cross-immunity with other coronaviruses, and local public health policies53,54. Genomic surveillance and continuous vaccine adaptation will remain essential tools for sustained disease control.
Conflicts of interest
The authors declared no conflicts of interest whatsoever.
Ethical considerations
Protection of human subjects and animals. The authors declare that no experiments on humans or animals were performed for this research.
Confidentiality, informed consent, and ethical approval. This study does not involve personal patient data, medical records, or biological samples, and does not require ethical approval. SAGER guidelines do not apply.
Declaration on the use of artificial intelligence (AI). The authors declare that no generative artificial intelligence was used in the writing or creation of the content of this manuscript.
