Introduction
Various comorbidities and risk factors have been associated with a higher likelihood of infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and with the development of severe forms of COVID-19 (Table 1). In addition, these factors have been observed to contribute to the persistence of symptoms after acute infection, known as long COVID-19 and post-COVID-19 syndrome1,2.
Table 1. Comorbidities and risk factors associated with SARS-CoV-2 infection
| Comorbidity/risk factor | Positive COVID-19 diagnosis | Severe disease | Mortality |
|---|---|---|---|
| Sex M:F1,2–5 | – | – | 2.8:1.7 OR, 1.69 (1.65-1.73) |
| Diabetes mellitus (prevalence, %)1,3–5 | 9-65% | 16.8-29.1% OR, 3.12 95% CI: 1.0-9.75 |
24.9% RR, 1.95 (1.41-2.49) |
| Cerebrovascular disease: Systemic arterial hypertension1,2–5 (prevalence, %) |
8.0% 14.3% 95% CI: 6.6-28.42 |
26.46% 47.65% OR, 1.97 95% CI: 1.40-2.77 |
RR, 2.14 (1.66-2.63)2 25.2% 47.9% |
| Cerebrovascular disease2 | RR, 2.43 (2.15-2.72)2 | ||
| Respiratory diseases: COPD1,3–5 (prevalence, %) |
3.7% | 17.28-25.4% OR, 6.42 95% CI: 2.44-16.9 |
RR, 1.98 (1.48-2.47)2 10.9% |
| Obesity6,7 | OR, 1.50 95% CI: 1.37-1.63 |
OR, 1.54 95% CI: 1.33-1.78 |
OR, 1.14 95% CI: 1.04-1.26 |
| Deep vein thrombosis8 Pulmonary embolism11 (prevalence, %) |
30% 18% |
– | – |
| Acute kidney injury9 (prevalence, %) | 10.6% | – | OR, 11.05 95% CI: 9.13-13.36 |
| Cancer2 | RR, 1.84 (1.24-2.43) | ||
| Smoking1,3,4,5,10 | – | OR, 1.96 95% CI: 1.36-2.83 |
OR, 1.18 (1.13-1.22)2 |
| Current smokers Former smokers |
6.98% – |
– OR, 3.29 95% CI: 1.51-7.18 |
– |
COVID-19, coronavirus disease 2019; COPD, chronic obstructive pulmonary disease; 95% CI, 95% confidence interval; OR, odds ratio; RR, relative risk; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; PE, pulmonary embolism.
The presence of comorbidities not only increases the risk of infection but also the likelihood of obtaining a positive PCR (polymerase chain reaction) test and developing antibodies, even in the absence of symptoms. Depending on the type of comorbidity, the risk may vary: symptomatic infection without pneumonia, need for hospitalization, mechanical ventilation, or death. Likewise, certain comorbidities may favor the development of additional complications such as thromboembolism or acute kidney injury. It is estimated that approximately 40% of individuals who develop SARS-CoV-2 infection have at least 1 comorbidity, and among those who die, around 74% had a preexisting condition1.
Pathophysiology of SARS-CoV-2 infection
SARS-CoV-2 is a virus that infects alveolar epithelial cells through the angiotensin-converting enzyme 2 (ACE2) pathway. This ACE2 receptor acts as a binding site for the spike (S) protein of the SARS virus (SARS-CoV). The modified S protein of SARS-CoV-2 has a significantly higher affinity for ACE2, with a binding probability 10 to 20 times greater than that observed with the S protein of the earlier SARS-CoV.
ACE2 is widely distributed in various organs, including the heart, vascular system, kidneys, lungs, and colon, among others. During SARS-CoV-2 infection, ACE2 expression in alveolar epithelial cells decreases, leading to increased levels of angiotensin II. This increase promotes vascular smooth muscle contraction, cellular proliferation, inflammation, and endothelial dysfunction3,4. In addition, viral replication produces an imbalance in the immune response mediated by T helper type 1 and type 2 lymphocytes, which may trigger the so-called “cytokine storm”3.
Comorbidities and increased risk of adverse events
Many of the comorbidities observed in patients with COVID-19 are characterized by chronic inflammatory processes. For example, patients with cardiovascular and cerebrovascular diseases exhibit persistent vascular damage, whereas those with COPD develop alveolar epithelial deterioration. These factors, when combined with the acute process of SARS-CoV-2 infection, significantly increase the risk of complications3.
The development of complications during SARS-CoV-2 infection depends on various factors, including the type of comorbidity, age, type of medications used (eg, nonsteroidal anti-inflammatory drugs [NSAIDs] and nephrotoxic agents, among others), viral load, and the integrity of host defense mechanisms.
Most comorbidities create a state in which defense mechanisms are impaired5.
The integrity of the respiratory mucosa, the proper functioning of the mucociliary mechanism, and innate defense systems in general constitute the first line of protection in previously exposed individuals. These innate mechanisms may be reinforced by adaptive immunity through antibodies and lymphocytes previously sensitized by vaccination, prior infection, or exogenous antibody administration. In cases of immunosuppression, greater viral replication during the early stages of infection is expected, which may translate into increased tissue damage and more severe clinical complications.
Age has been identified as one of the most important predictive factors for severe complications and mortality from COVID-196; as age increases, the number of comorbidities rises and outcomes worsen. However, several statistical models have allowed differentiation between the independent effects of age and comorbidities. The rate of SARS-CoV-2 infection triples after 18 years of age; the hospitalization rate increases up to 15-fold after 40 years of age; and mortality is 45 times higher in individuals > 30 years3.
In databases such as the Mexican COVID-19 registry, an additive effect of comorbidities has been observed, meaning that the number of comorbidities is a strong predictor of mortality (Fig. 1). For example, patients with severe disease more frequently had at least 1 comorbidity: hypertension (odds ratio [OR], 2.36), respiratory diseases (OR, 2.46), and cardiovascular diseases (OR, 3.42)6–10. Similarly, age has been associated with a higher risk of developing post-COVID-19 syndrome, with an OR of 1.21 (95% CI, 1.11-1.33)11.
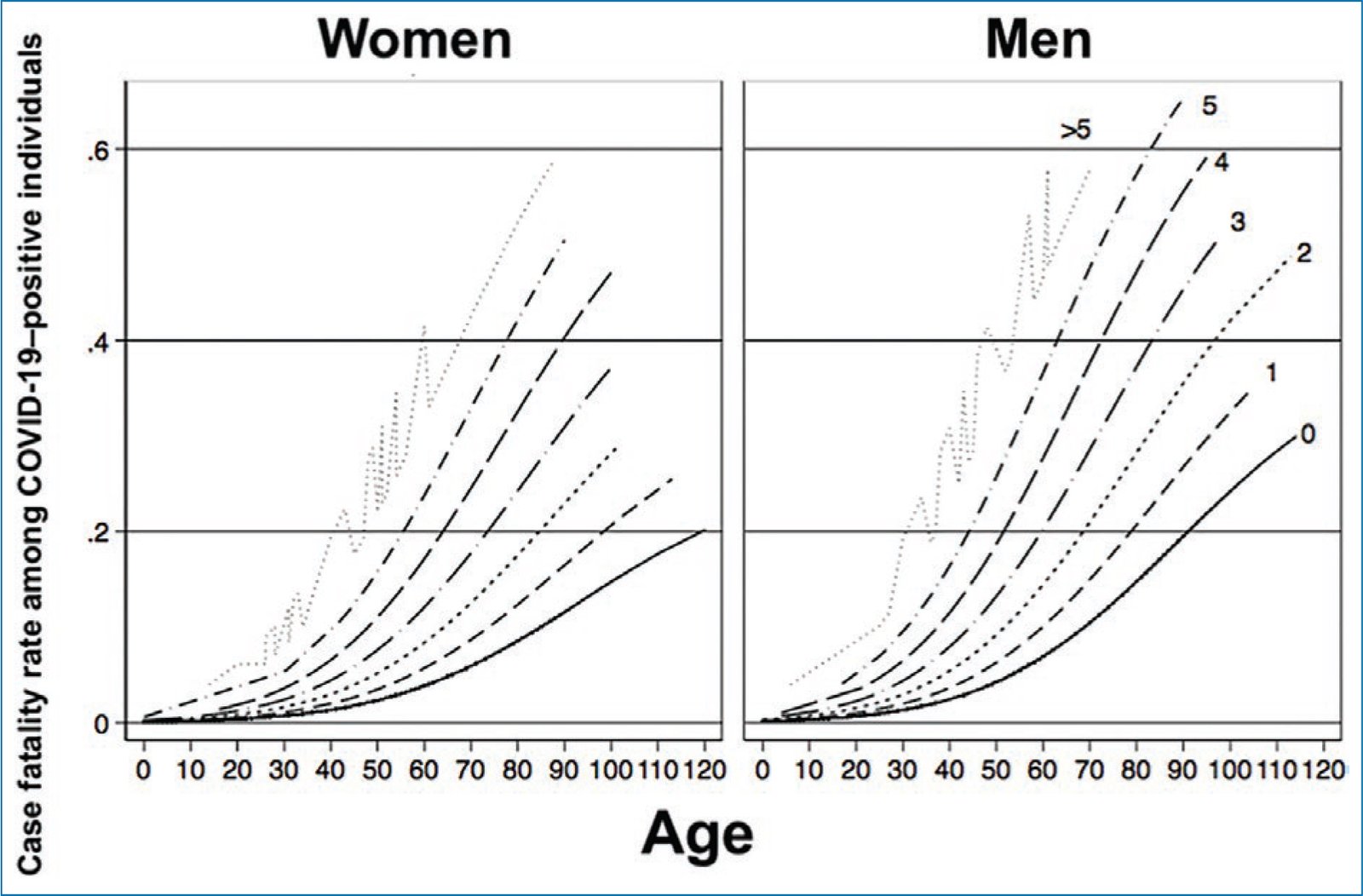
Figure 1. Association between case fatality and number of comorbidities in patients with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection in Mexico.
Male sex has been associated with a higher risk of requiring admission to intensive care units, with an OR of 1.55 (95% CI, 1.02-2.36)12, as well as an increased risk of mortality3. Women appear to have lower susceptibility to severe SARS-CoV-2 infection, attributed to the influence of sex hormones, which play an important role in both innate and adaptive immunity3. However, this trend is reversed in post-COVID-19 syndrome, where female sex has shown a higher risk, with an OR of 1.56 (95% CI, 1.41-1.73) according to a systematic review11.
The association between obesity and SARS-CoV-2 infection, as well as its negative impact on clinical prognosis, has been documented in several studies2,5,13. Obesity increases the risk of obtaining a positive PCR test for SARS-CoV-2, with an OR of 1.50 (95% CI, 1.37-1.63); moreover, the higher the body mass index (BMI), the greater the probability of a positive result. Similarly, obesity has been associated with a higher risk of hospitalization and intensive care unit admission, with ORs of 1.54 (95% CI, 1.33-1.78) and 1.48 (95% CI, 1.24-1.77), respectively, and a higher risk of death (OR, 1.14; 95% CI, 1.04-1.26)8.
Coronary artery disease, stroke, and heart failure have shown an incidence 2 to 3 times higher in patients requiring intensive care unit admission, and mortality rates of up to 10.5% have been reported in individuals with these comorbidities1,5.
Similarly, the presence of diabetes mellitus has been associated with a significant increase in mortality among patients with SARS-CoV-2 infection, as shown in a recent meta-analysis reporting a relative risk (RR) of 1.95 (95% CI, 1.41-2.49). In the case of pulmonary diseases, a similar pattern has been observed, with a higher risk of mortality (RR, 1.98; 95% CI, 1.48-2.47)2.
Certain comorbidities have been identified as increasing the risk of developing more severe SARS-CoV-2 infection, with high and consistent levels of evidence. These include chronic kidney disease, chronic obstructive pulmonary disease (COPD), heart failure, coronary artery disease, cardiomyopathies, obesity, pregnancy, smoking, solid organ transplantation, and type 2 diabetes mellitus1,8. On the other hand, comorbidities associated with a higher risk of infection after contact with a confirmed case include systemic hypertension, chronic respiratory diseases, diabetes, and cerebrovascular diseases9.
Among the comorbidities described as risk factors for developing post-COVID-19 syndrome are ischemic heart disease, immunosuppression, diabetes, COPD, anxiety, depression, asthma, and having required hospitalization during the acute infection. On the other hand, a protective factor for the development of post-COVID-19 syndrome is having received two doses of COVID-19 vaccination11.
The incidence rate of deep vein thrombosis also increases in the context of SARS-CoV-2 infection and has been associated primarily with advanced age and higher BMI. This phenomenon is largely attributed to thrombophilia due to dysregulation of the hemostatic system, as well as prolonged immobilization in many patients. Pathologic studies have demonstrated a higher prevalence of thrombosis and microangiopathy in patients with SARS-CoV-2 infection vs those with H1N1 influenza14.
Chronic kidney disease represents a significant risk factor that more strongly influences mortality than the total number of comorbidities present5,15,16. Several systematic reviews have estimated an increased risk of mortality in patients with renal involvement2. The mechanism of injury is attributed in part to direct damage to intrinsic renal cells, as SARS-CoV-2 acts as a cytopathic virus. Epithelial cells of the renal proximal tubules exhibit high expression of the ACE2 receptor, which facilitates viral binding to this cell type and contributes to greater renal injury15.
Smoking, vaping, and the presence of comorbidities
Nicotine use, regardless of its form – whether through combustible cigarettes, electronic cigarettes (vaping devices), or heated tobacco products – represents a significant risk to the pulmonary and cardiovascular systems17. Nicotine administration, through either combustible cigarettes or electronic devices, has been shown to increase systolic and diastolic blood pressure, peripheral pulse pressure, and heart rate18. Over the long term, these changes induced by continuous nicotine exposure may lead to permanent cardiovascular dysfunction, particularly in predisposed individuals or those with preexisting diseases.
Various mechanisms associated with tobacco use contribute to these effects, including increased heart rate and myocardial contractility, inflammation, endothelial dysfunction, thrombus formation, and reduced serum levels of high-density lipoprotein cholesterol (HDL-C). Moreover, these alterations increase oxidative stress and systemic inflammation19. In the case of electronic cigarette or vaping device use, an additional acute inflammatory response is triggered by several additives present in these devices, such as propylene glycol, glycerin, and flavoring agents.
Accordingly, the association between smoking and the development of cardiovascular diseases has been widely described in the literature19,20, and similar findings have been reported with the use of electronic devices21. Moreover, recent studies show that reducing tobacco consumption – and even more so, complete smoking cessation – has an impact on lowering the risk of comorbidities and death20,22,23.
Smoking, vaping, and COVID-19
Various cellular signaling pathways and genes have been identified that are affected both by nicotine use – whether through conventional cigarettes, electronic cigarettes, or other forms of nicotine delivery – and by SARS-CoV-2 infection and disease progression24. ACE2 receptors are upregulated in the airway epithelium of smokers, especially on the surface of type II pneumocytes25, with greater ACE gene expression observed in samples from smokers compared with never-smokers, and increased ACE2 receptor expression in the lungs of smokers with COPD as demonstrated by immunohisto-chemistry26. The previously described loss of homeostasis and the facilitated binding of the SARS-CoV-2 spike protein to epithelium due to increased ACE2 receptor expression confer a higher risk of developing viral infection such as SARS-CoV-210.
A retrospective case-control study based on electronic health records of 73,099,850 patients, of whom 12,030 had confirmed COVID-19, reported that individuals with a recent diagnosis of substance use disorder had a significantly higher risk of contracting COVID-19 (adjusted OR, 8.699; 95% CI, 8.411-8.997; p < 10-30), particularly in the case of tobacco use (adjusted OR, 8.222; 95% CI, 7.925-8.530; p < 10-30)27. Furthermore, a meta-analysis demonstrated a higher risk of mortality among individuals with a history of smoking compared with never-smokers (OR, 1.18; 95% CI, 1.13-1.22)2, as well as a greater risk of developing post-COVID-19 syndrome among smokers compared with never-smokers11.
In particular, dual users – those who use both conventional tobacco and electronic cigarettes – have up to a 30% higher risk of COVID-19 infection and disease progression compared with nonusers28,29. Suppression of gene activity involved in immune and inflammatory responses in nasal epithelial cells has been documented in individuals who vape30. Likewise, smoking and/or vaping increase oxidative stress and pulmonary inflammatory responses, making smokers and vapers more susceptible to bacterial and viral infections31.
Vaping has increasingly been associated with the development and exacerbation of pulmonary diseases. EVALI (e-cigarette or vaping product use – associated lung injury) is characterized by acute lung injury, acute fibrinous pneumonitis, diffuse alveolar damage, or pneumonia accompanied by bronchiolitis32,33 and increases the risk of COVID-19 complications among vapers. Dysregulation of airway lipids in users of electronic nicotine delivery systems (ENDS) may render them more susceptible to SARS-CoV-2 infection34. Therefore, it is important to strengthen the evidence that vaping directly affects the immune system and harms health35.
Furthermore, Gaiha et al. identified an association between youth smoking, electronic cigarette use, and COVID-19. They reported that vaping and dual use of conventional and electronic cigarettes – the most common pattern of use – were associated with a greater likelihood of being diagnosed with COVID-19 and experiencing symptoms. A COVID-19 diagnosis was 5 times more likely among those who had ever used electronic cigarettes and 6.8 times more likely among dual users in the past 30 days. In addition, symptoms were 4.7 times more likely among dual users in the past 30 days (Table 1)36.
Conclusions
Identifying factors associated with a higher incidence of infection and the development of severe forms of disease is essential for designing specific public health programs and strategies. These actions help reduce both incidence and poor prognosis, as well as associated mortality. Smoking, recognized as a disease with multiple harmful effects on health, should be considered a relevant risk factor in the context of COVID-19, as it increases the likelihood of complications and adverse outcomes.
Funding
This work did not receive any funding.
Conflicts of interest
The authors declared no conflicts of interest whatsoever.
Ethical considerations
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this research.
Confidentiality, informed consent, and ethical approval. The study does not involve personal patient data and does not require ethical approval. SAGER guidelines do not apply.
Declaration on the use of artificial intelligence. The authors declare that they did not use any type of generative artificial intelligence in drafting this manuscript.
