“Bronchial anthracosis” was the term initially used to describe blackish-blue discoloration of the bronchial mucosa due to carbon deposition. Bronchoscopic observations indicate that biomass exposure is associated with a higher frequency of bronchial anthracofibrosis (30.4%) vs tobacco exposure (3.7%)1.
Bronchial anthracofibrosis is characterized by areas of bronchial stenosis in approximately 80% of cases. Multifocal bronchial narrowing may involve segmental and lobar bronchi and may extend contiguously to the distal trachea. These changes typically develop at sites of turbulent airflow2. Associated findings may include calcified lymphadenopathy and atelectasis. The so-called anthracotic triad consists of hyperdense lymph nodes, atelectasis, and hyperdense pulmonary parenchyma3 (Figure 1).
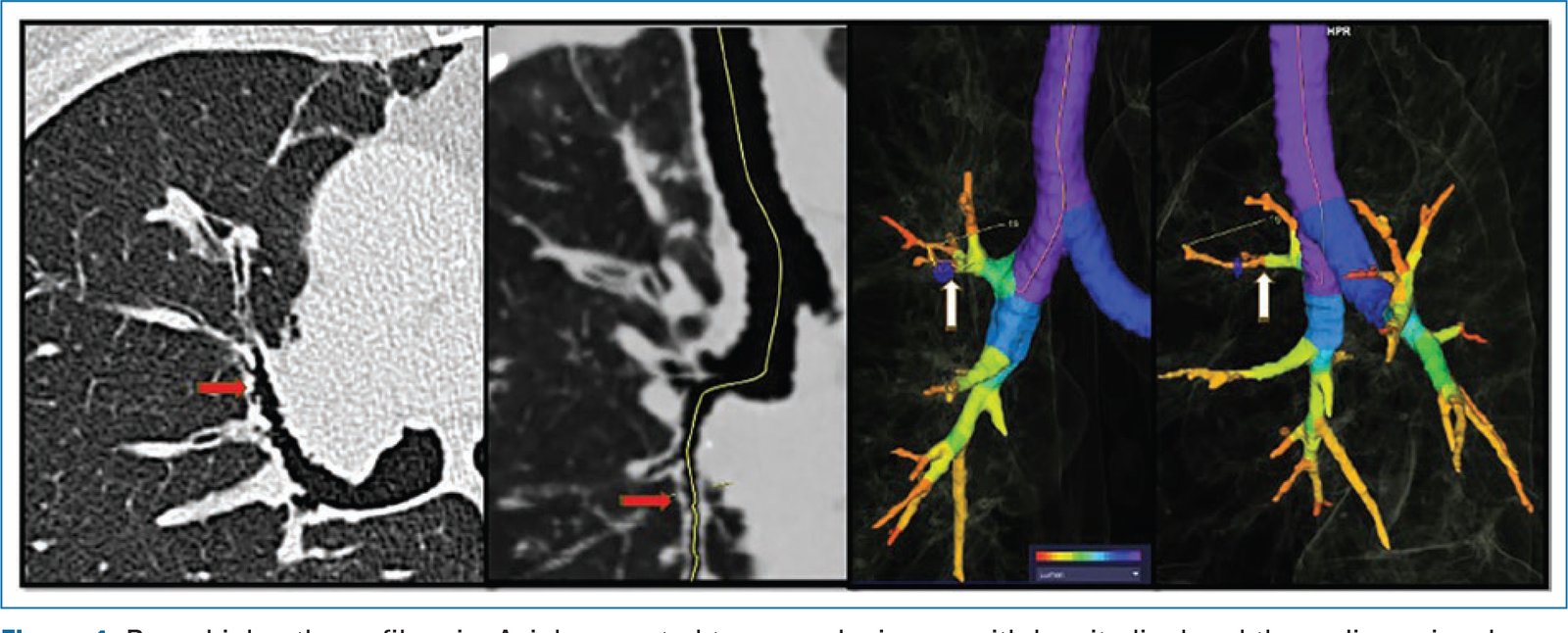
Figure 1. Bronchial anthracofibrosis. Axial computed tomography image with longitudinal and three-dimensional reconstruction of the segmental airway. Arrows indicate areas of luminal narrowing associated with wall thickening and irregularity of the internal margin.
Funding
This study did not receive specific funding from public sector agencies, commercial entities, or nonprofit organizations.
Conflicts of interest
The author declared no conflicts of interest whatsoever.
Ethical considerations
Protection of human and animal subjects. The authors declare that the procedures followed were in accordance with the ethical standards of the responsible human experimentation committee and the World Medical Association Declaration of Helsinki. The procedures were authorized by the institutional ethics committee.
Confidentiality, informed consent, and ethical approval. This study does not involve personal patient data and does not require additional ethical approval. The SAGER guidelines were not applicable.
Declaration on the use of artificial intelligence. The authors declare that no generative artificial intelligence tools were used in the preparation of this manuscript.
