Introduction
Paraquat intoxication is a public health problem due to its high toxicity. It is a widely used herbicide in agriculture, associated with serious complications such as pulmonary fibrosis1. The pathogenesis includes inflammatory processes and oxidative stress that lead to impairment of lung function2. It causes significant cellular damage through the generation of reactive oxygen species, contributing to the development of fibrosis3. In the Colombian context, a recent study has addressed the challenges faced by the country in relation to paraquat poisonings, highlighting the urgent need to improve prevention and management strategies4. The high rate of intoxications has made evident the lack of effective measures to protect exposed communities5. The inflammatory response and fibrosis resulting from paraquat exposure underline the importance of understanding the mechanisms involved in this pathology6,7. The effects include a reduction in respiratory capacity and a deteriorated quality of life8. Furthermore, the management of this intoxication must be adapted to the specific characteristics of each case9. The literature suggests that safety measures and education are crucial to reduce exposure and the risk of intoxication10. However, prevention remains an essential component. Research on signaling pathways and therapeutic mechanisms is ongoing and offers hope for the development of more effective treatments11.
Case report
A 17-year-old male patient, without significant past medical history, from Orito, Putumayo, in southern Colombia. The patient was admitted with acute paraquat (Gramoxone®) intoxication after the voluntary ingestion of approximately 100 ml. According to the degree of intoxication, the prognosis is established (Table 1). In this case, the ingestion of 100 mL of paraquat, equivalent to 20 g of paraquat, that is, 289.86 mg/kg calculated with a weight of 69 kg, corresponds to a severe intoxication with a 100% mortality rate in 1 to 5 days11.
Table 1. Prognosis according to the degree of paraquat intoxication
| Degree of intoxication | Amount of paraquat | Signs |
|---|---|---|
| Mild | < 10 mL at 20% P/V (< 20 mg/kg) | GI symptoms, mild renal failure. Recovery without sequelae highly probable in 100% of cases. |
| Moderate-to-severe | 10-20 mL at 20% P/V (20 to 40 mg/kg) | GI symptoms, renal failure, hepatitis, pulmonary fibrosis, which may lead to death. 30-60% mortality after the fifth day. |
| Fulminant | > 20 ml at 20% P/V (> 40 mg/kg) | Rapid onset multi-organ failure, shock, or perforation of the gastrointestinal tract. 100% mortality in 1 to 5 days. |
Adapted from Marín and Berrouet¹¹.
At the time of admission, general decontamination measures were taken. The treatment included N-acetylcysteine (200 mg every 6 hours orally), prednisone (50 mg every 24 hours orally), enalapril (5 mg every 12 hours), and respiratory therapy (every 8 hours), consisting of N-acetylcysteine plus respiratory incentive. Additionally, formoterol/budesonide (4.5/160 µg every 12 hours) and piperacillin-tazobactam (4 g every 6 hours intravenously) were administered. This regimen was implemented to address the patient’s clinical needs.
The patient was in poor general condition, with symptoms of dysphagia, odynophagia, diaphoresis, nasal flaring, and use of accessory muscles even at absolute rest. Physical examination revealed emphysema in the left axilla, and on auscultation, added sounds like rhonchi in both lung fields. Arterial blood gas analysis reported a compensated metabolic acidosis, with mild hypokalemia, elevated anion gap, and hypoglycemia. The PAFI index decreased consistently, indicating a progressive deterioration in the patient’s oxygenation over time.
During the length of stay, there was a progressive elevation of azotemia, with increased creatinine and blood urea nitrogen, evidencing renal failure with indications for hemodialysis. The initial radiological images did not show respiratory alterations; however, in subsequent studies, alterations in pulmonary morphology with bilateral basal laminar atelectasis, central peribronchial thickening, and left basal irregular opacities suggestive of alveolar occupation were observed (Fig. 1). Computed tomography showed parenchymal consolidations in the lung bases with air bronchogram and alveolar opacities with a ground-glass pattern in the upper lobes, the middle lobe, and the lingula, suggesting a pulmonary inflammatory process (Fig. 2).
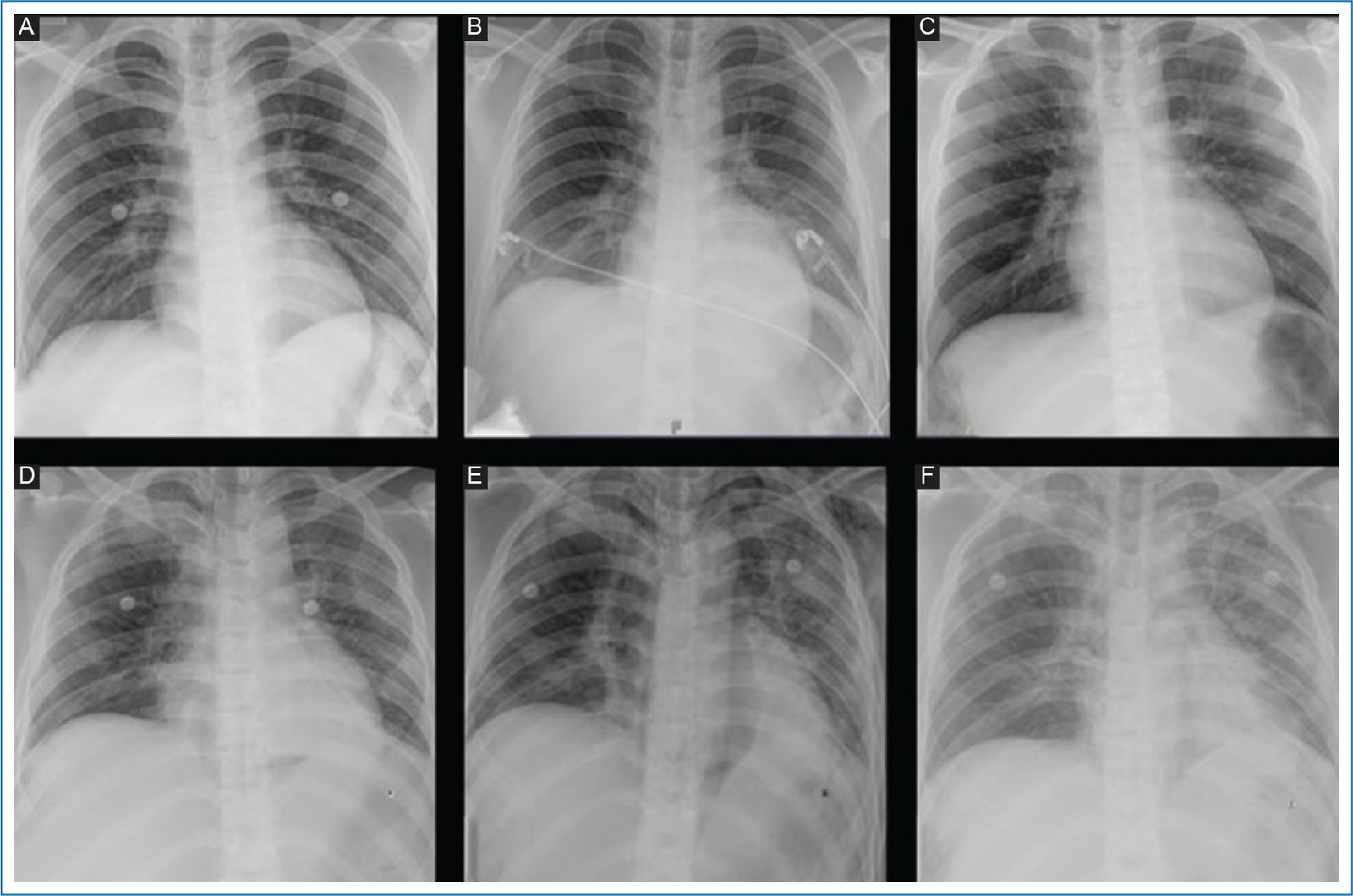
Figure 1. Radiological findings. A: satisfactory pleuropulmonary transparency, without evidence of consolidations or interstitial or alveolar opacities; free pleural spaces. B: bilateral basal laminar atelectasis. C: parahilar and bibasal interstitial opacities. D: left basal opacity suggestive of alveolar occupation. E: suggestive image of superior and inferior pneumomediastinum with retroperitoneal extension; left basal subsegmental atelectasis; bilateral cervical and left thoracic emphysema. F: central peribronchial thickening associated with left basal irregular opacities, suggesting alveolar occupation; left axillary emphysema.

Figure 2. Tomographic findings. A (1-2): parenchymal consolidations in the lung bases with air bronchogram; alveolar opacities with a ground-glass pattern in the upper lobes, the middle lobe, and the lingula, suggesting inflammatory involvement; consider multilobar pneumonia. B (1-2): findings in the lung parenchyma suggestive of changes due to a multilobar pneumonic process; correlate with medical history.
The patient experienced desaturation episodes with a torpid progression that included severe hypoxemia. Initially, he required supplemental oxygen with a high-flow nasal cannula, later evolving to non-invasive mechanical ventilation. Due to the progressive deterioration of respiratory function, orotracheal intubation and invasive mechanical ventilation were performed. Despite the management implemented to delay pulmonary damage, the clinical picture was complicated by bacterial pneumonia and a marked deterioration of respiratory function, requiring permanent oxygenation.
The patient was eligible for lung transplantation due to refractory respiratory failure, progression of pulmonary damage despite optimal treatment, and lack of response to conventional therapy.
Discussion
The presented case underscores the severity of paraquat intoxication and the need for greater awareness of the risks associated with this herbicide. Despite advances in medicine, mortality from paraquat poisoning remains high. Coordinated efforts are required to prevent these intoxications and develop new therapies to improve the prognosis of affected patients.
Paraquat intoxication represents a serious public health problem, especially in agricultural communities. In the national and international literature, cases with similar clinical presentations and outcomes have been reported. Studies have documented a high mortality rate in patients with ingestions exceeding 20 mg/kg, with progressive deterioration of pulmonary and renal function. The use of therapeutic strategies such as immunosuppression and hemoperfusion has also been described, with variability in clinical outcomes.
Regarding lung transplantation in patients with paraquat intoxication, there is significant controversy, especially when the case is related to a suicide attempt. Some reports suggest that these patients may not be optimal candidates due to the high risk of recurrence of the suicide attempt and the complexity of the procedure. However, in other cases, successful transplants have been documented in patients with respiratory failure secondary to paraquat intoxication, generating a debate on the selection criteria and the need to evaluate each case individually.
Conclusions
This case of acute paraquat intoxication in a 17-year-old patient shows the high toxicity of the herbicide and the associated severe complications, including atelectasis, pneumonia, and severe lung damage, along with renal failure. Despite intensive management, the patient suffered progressive deterioration of respiratory function and desaturation episodes, complicated by bacterial pneumonia. This case highlights the urgent need to improve prevention and education on paraquat intoxications, as well as the importance of early interventions and advanced treatments. The consideration for lung transplantation underscores the severity of the damage and the need for comprehensive medical care.
Funding
None declared.
Conflicts of interest
The authors declared no conflicts of interest whatsoever.
Ethical considerations
Protection of people and animals. The authors declare that no experiments were conducted on humans or animals for this research.
Confidentiality, informed consent, and ethical approval. The authors have followed the confidentiality protocols of their institution, obtained informed consent from the patients, and have the approval of the Ethics Committee. The SAGER guidelines have been followed according to the nature of the study.
Declaration on the use of artificial intelligence. The authors declare that no type of generative artificial intelligence was used in the writing of this manuscript.