Introduction
Obstructive sleep apnea (OSA) is a condition exclusive to sleep. It is defined as partial or complete collapses of the upper airway (UA), associated with hypoxemia, hypercapnia, hypoventilation and/or microarousals, snoring, fragmented nonrestorative sleep, and excessive daytime sleepiness (EDS), among other symptoms. It correlates with increased cardiovascular risk, metabolic and cognitive alterations, and worsening quality of life in affected individuals1–2. OSA has a global prevalence of 4% to 30%3.
According to pathophysiology, polysomnographic characteristics, and clinical presentation, various OSA phenotypes have been identified. One of them, known as positional OSA (POSA), describes patients whose obstructive respiratory events are more frequent in the supine position. It is observed in Caucasian and Asian populations, in younger, leaner individuals, with lower body mass index (BMI), lower blood pressure, and a less severe apnea-hypopnea index (AHI); they experience fewer awakenings and less snoring, with better sleep duration and efficiency4,5. The prevalence of POSA ranges between 50% and 60% of patients with OSA6.
Treatment options for POSA include positive airway pressure (PAP), mandibular advancement devices (MADs), upper airway surgery, certain medications, and positional therapy (PT). These treatments are specific and/or complementary depending on the predominant phenotype and endotype in each patient, with notable variability in efficacy. This narrative literature review aims to describe and promote medical recognition of the characteristics of patients with POSA.
History and definition of positional obstructive sleep apnea
POSA is considered a specific OSA phenotype. It is defined by the exclusive or significantly predominant occurrence of apneas and hypopneas in a particular position, that is, the worst position (Fig. 1, Table 1); however, specific diagnostic thresholds vary in the published literature.
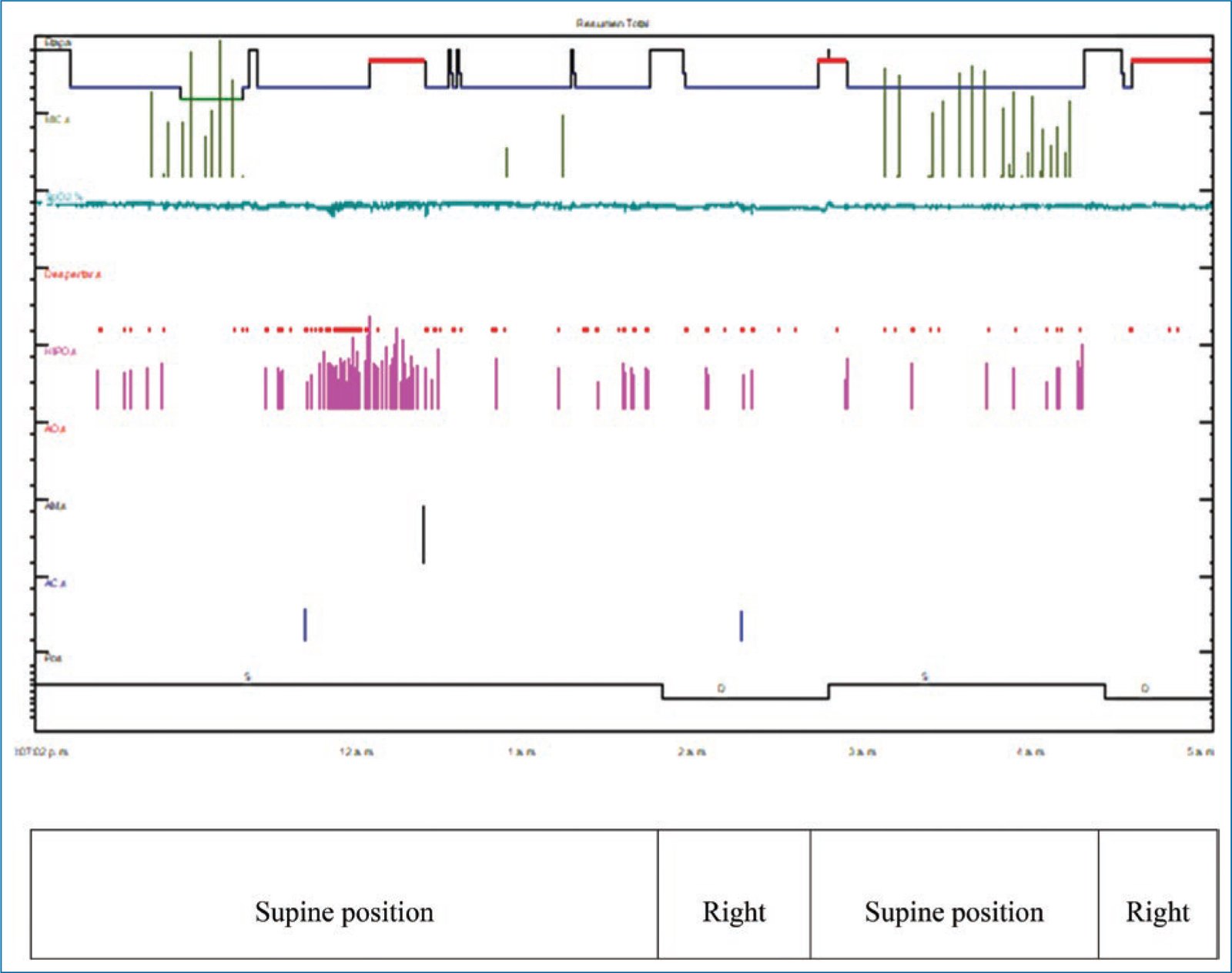
Figure 1. Positional obstructive sleep apnea. Polysomnography with clear predominance of obstructive apneas and hypopneas during the supine position, independent of sleep stage.
Table 1. Postural obstructive sleep apnea (POSA): distribution of body positions
| Position | Duration (min) | Sleep (%) | REM (%) | Oxygen desaturation (events) | Apnea-hypopnea index (No./h) |
|---|---|---|---|---|---|
| Supine | 307.8 | 94.4 | 8.6 | 117 | 17.1 |
| Right | 96.7 | 86.3 | 33.6 | 21 | 4.3 |
| Left | |||||
| Prone |
A higher-than-normal apnea – hypopnea index is observed in the supine position.
REM: rapid eye movement sleep.
Cartwright was the first to suggest differentiating between patients with POSA and nonpositional OSA (non-POSA), arbitrarily defining POSA as a 50% or greater difference in AHI between the supine and nonsupine positions7. Since then, different authors have proposed multiple modifications to increase diagnostic specificity and improve therapeutic efficacy (Table 2)7–12.
Table 2. Definitions of postural obstructive sleep apnea (POSA)
| Author | Year | Definition |
|---|---|---|
| Cartwright7 | 1984 | Total AHI > 5/h, ≥ 50% difference in AHI between the supine and non-supine positions |
| Marklund et al.8 | 1998 | AHI ≥ 10/h in supine + lateral AHI < 10/h in lateral position |
| Permut’s9 | 2005 and 2010 | AHI < 5/h in the non-supine position plus a reduction in AHI > 50% between supine and non-supine positions. Difference between supine-predominant positional apnea (AHI ≥ 5/h in non-supine position) and supine-exclusive positional apnea (AHI < 5/h in non-supine position) |
| Bignold et al.10 | 2011 | Total AHI ≥ 15/h, supine AHI ≥ double the non-supine AHI, AHI < 15/h in non-supine. Minimum 20 minutes of sleep in supine and lateral positions. |
| Levendowski et al.11 | 2014 | Total AHI/non-supine AHI > 1.5 |
| Frank et al.12 | 2015 | Introduces 3 categories (APOC) considering best and worst positions. Minimum 10% of total sleep time in both best and worst positions |
APOC: Amsterdam Positional OSA Classification; AHI : apnea-hypopnea index per hour.
Bignold et al defined POSA as a total AHI ≥ 15 events/h, with at least twice as many events in the supine vs the nonsupine position, a nonsupine AHI ≤ 15 events/h, and at least 20 minutes of sleep recorded in each evaluated position10; this definition is specific and consistent with the American Academy of Sleep Medicine (AASM)13.
Frank et al incorporated the definitions of best and worst position along with a minimum recording time per position12. This was complemented in 2016 by the Amsterdam Positional OSA Classification (APOC), focused on improving patient selection and, consequently, the effectiveness of positional retraining therapy (PRT), establishing 3 categories6 (Table 3).
Table 3. Amsterdam Positional OSA Classification and its impact on selection of positional therapy
| Classification | Definition | Treatment implication |
|---|---|---|
| APOC I | AHI in the most favorable sleep position < 5/h (exclusive POSA) | Positional therapy or positional retraining as monotherapy |
| APOC II | AHI in the most favorable sleep position reduces OSA severity | Positional therapy or positional retraining as adjunctive therapy |
| APOC III | Total AHI ≥ 40, with ≥ 25% reduction in AHI in the most favorable position | Consider positional therapy or positional retraining as adjunctive therapy |
APOC: Amsterdam Positional OSA Classification. Adapted from Berri et al.13
Epidemiology and clinical characteristics
OSA is the most prevalent sleep-related breathing disorder, affecting 12.5% of men and 5.9% of women in the general population; 49.7% of men and 23.4% of women > 40 years have an AHI > 15 events/h14. The prevalence of POSA varies according to age, ethnicity, AHI severity, and the diagnostic criteria applied. Predominant POSA (pPOSA) is estimated to occur in 50% to 60%15–17, whereas exclusive POSA (ePOSA) occurs in 20% to 35%11,18 (Fig. 2).
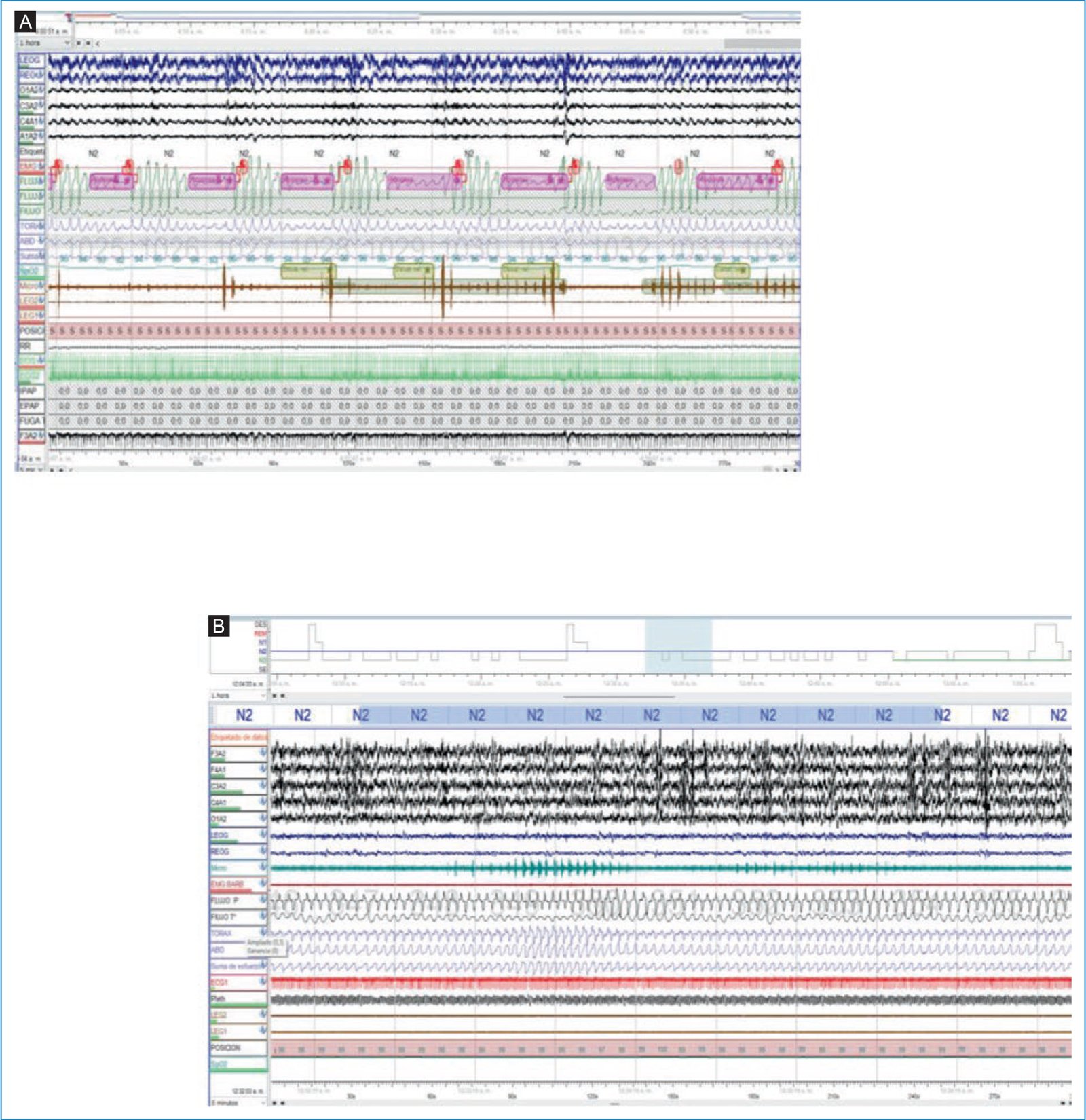
Figure 2. Exclusive positional obstructive sleep apnea. Two 5-minute epochs from a baseline polysomnography study are shown. A: patient in the supine position with snoring and hypopneas associated with desaturation and microarousals in N2. B: patient in the left lateral decubitus position with persistent snoring, without obstructive respiratory events or desaturation in N2.
Studies suggest a higher prevalence of POSA in Asian populations (67%-75%)19,20, as well as in younger, leaner patients with fewer comorbidities15,16,21; mean age ranges from 49.5 to 52.9 years vs 54.9 to 59.2 years in non-POSA9,16. Furthermore, there is an inverse relationship between OSA severity and POSA prevalence. Mador et al reported a POSA prevalence of 49.5% in mild OSA, 19.4% in moderate OSA, and 6.5% in severe OSA19. POSA is more frequent in men than in women, with a ratio of 11.1:1 across severity grades and 2.6:1 in mild and moderate OSA; this discrepancy may be explained by the higher proportion of men with severe OSA18,22.
Patients with POSA tend to have a lower BMI (29.331.6 kg/m2) vs those with nonpositional OSA (31.938 kg/m2)9,16,18. The BMI difference is particularly notable in patients with exclusive POSA, even after controlling for AHI. These patients also exhibit smaller neck and waist circumferences, more favorable Mallampati classification, lower prevalence of hypertension, higher oxygen saturation nadir, and lower glucose levels – factors independently associated with non-POSA9,23.
Clinically, patients with non-POSA have higher scores on the Epworth Sleepiness Scale24, STOP and STOPBang questionnaires25, and the Berlin questionnaire18,26, likely associated with higher AHI, desaturation index, microarousals, reduced N3 and REM sleep stages, and lower sleep efficiency7,20. In contrast, snoring in patients with POSA is reported to be more frequent and more intense in the supine position27,28, an important consideration when selecting PT alone or combined in patients who continue to snore in favorable positions.
Pathophysiology
As a phenotypic variant of OSA, POSA has multiple pathogenic factors, including anatomical conditions, critical closing pressure (Pcrit), lung volume and tracheal traction, upper airway dilator muscle activity, ventilatory stability, and arousal threshold29. The interaction and balance among these factors at different stages and times determine event occurrence, and understanding them is key to identifying specific treatments.
Anatomy
The size, shape, and position of bony structures (maxilla, mandible, cervical vertebrae) and soft tissues (nasal valve, turbinates, adenoids, soft palate, uvula, palatopharyngeal and palatoglossal muscles, palatine tonsils, lingual tonsils, tongue, epiglottis, fat pads), as well as upper airway tone characteristics, influence upper airway collapse in patients with OSA. This is particularly true in the supine position, as demonstrated by static and dynamic imaging modalities performed during wakefulness and sleep, evaluating different body positions and head rotation, despite methodological differences and variability in populations and sleep stages studied30–32.
Individuals without OSA typically show changes in upper airway area when moving from sitting to supine but do not exhibit changes from supine to lateral positions32. In contrast, patients with OSA demonstrate a small but significant reduction in anteroposterior retropalatal space and in oropharyngeal and hypopharyngeal area in the supine position33. Patients with POSA exhibit a more posterior mandibular position and greater lateral area in the retropalatal space, as well as in the oropharynx and hypopharynx34–37. Although few studies have compared upper airway behavior during drug-induced sleep endoscopy, POSA patients appear to have less concentric retropalatal collapse and greater collapse at the epiglottic level rather than at the tongue base38–39.
It has been hypothesized that the increased lateral diameter in the oropharynx and hypopharynx observed in POSA patients reduces the likelihood of obstructive events in the lateral position, compensating for the decreased anteroposterior area characteristic of OSA patients and associated with more favorable conditions in other factors such as lung volumes.
Additionally, it has been discussed whether nasal resistance derived from mechanical nasal obstruction – by increasing the collapsibility of the “tube” of the UA-could be involved in how a non-POSA patient might become a POSA patient once those obstructive points are treated, representing an efficient alternative management strategy to PAP therapies.
Lung volumes
Lung volume is an important factor in the generation of OSA and is related to the stability of UA structures through the caudal traction exerted by the trachea, as well as to the critical closing pressure of the UA (Pcrit)40–42. In humans, changing from upright posture to the supine position implies a reduction in functional residual capacity (FRC), total lung capacity, expiratory reserve volume (ERV), and vital capacity, without changes in residual volume43–45. These volumes are also affected by BMI; thus, patients with BMI 25 kg/m2 to 30 kg/m2 show a linear decrease in FRC and ERV when moving from sitting to supine46. Information is still lacking regarding these volumes during positional changes from lateral decubitus to supine47–49. As noted, changes in lung volumes affect UA stability during sleep in the supine position43–46,50,51. Stanchina et al. demonstrated in 19 healthy young adults that a 600-mL reduction in end-expiratory lung volume increases the pharyngeal critical closing pressure by 1.1 cm H2O, making the UA collapsible despite increased genioglossus activation41 – comparable to the observation by Tagaito et al. that a 750-mL increase in end-expiratory lung volume reduces the pharyngeal critical closing pressure by 1.2 cm H2O52. Stadler et al., using an abdominal cuff, showed that increased intra-abdominal pressure during sleep in individuals with obesity (mean BMI, 34.5 kg/m2) produces a 530-mL decrease in endexpiratory lung volume and a 1.4 cm H2O increase in pharyngeal critical closing pressure, demonstrating the interaction among increased BMI, decreased lung volumes, and increased UA collapsibility53.
Critical closing pressure
Functional anatomic impairment of the UA is measured by Pcrit54,55. A supra-atmospheric or “positive” Pcrit increases susceptibility to OSA vs “negative” Pcrit values, that is, negative intraluminal (suction) pressures56–58. Pcrit varies due to many factors, including bony and soft-tissue configuration, BMI, sleep stage, and body and head position59,60. Currently, no studies have specifically assessed Pcrit in patients with OSA and POSA; however, it is presumed that POSA patients have more significant position-related changes in Pcrit, associated with predisposing anatomic conditions and marked changes in lung volumes.
Positional therapy and positional retraining
PAP therapy remains the reference treatment for OSA; however, new therapeutic approaches have emerged, and in patients with POSA, several types of treatments have been described: PAP therapy, MADs, surgical management, PT, and positional therapy and positional retraining therapy (PRT)61,62. PT is the treatment of choice for these patients, either as monotherapy or combined with other therapeutic strategies. It consists of preventing the patient from adopting the worst sleeping position – usually supine – through different methods.
The first description recorded in the literature (1984) appears in a letter written by a patient’s wife, describing how she mitigated her husband’s snoring by sewing a pocket on the back of his pajama shirt and inserting a tennis ball. This is known as the “tennis ball technique” (TBT). Although small case reports have shown this technique to be effective in preventing the supine position, poor long-term adherence has been attributed to discomfort, pain, and multiple awakenings it may cause63–65.
Modifications using objects such as special pillows and vests with pads have been proposed66–68, but longterm adherence remains low, and these treatments are unable to objectively measure actual usage time and nonsupine positioning. In response, PRT emerged with the aim of inducing repositioning into a favorable position through devices placed on different body regions that generate subtle vibration. This approach has been shown to be more efficient, effective, and comfortable long term12,69,70. PRT may be curative in some cases of exclusive POSA (ePOSA) according to the APOC classification, in which APOC I are truly positional, and may be adjunctive in other cases.
De Vries et al.63 evaluated PT effectiveness in 53 participants; 40 underwent follow-up polysomnography (PSG) using either a commercial chest band or a homemade device. They found a significant reduction in in the 12-week AHI among POSA patients (mean AHI, 14.5 to 5.9 events/h; p < .001), thus corroborating prior case reports.
Although few studies are available62,63,65, poor longterm adherence to this type of therapy has been demonstrated. De Vries et al. reported that 65% of patients had discontinued treatment by 13 months63. Oksenberg et al. reported 38% adherence at 6 months62, and Bignold et al. observed < 10% use of PT with TBT at 30 months65. In 2012, Heinzer et al.71 evaluated real-world PT use with a modified TBT combined with actigraphy in 16 patients over 3 months: mean use was 8 hours (range, 3.8-10.2 h); 10 patients used the device for > 80% of the time and 13 for > 60%. These findings highlight clear disadvantages of TBT vs other PT methods, particularly PRT.
Positional retraining therapy or new positional therapy
New technologies in this area have led to multiple reports over the past decade describing the efficacy and long-term follow-up of small vibratory devices with integrated accelerometers, positioned on the anterior chest, cervical region, or forehead. Their objective is to prompt the patient to change position through escalating vibrations, constituting PRT67,72–75. Advantages include better adherence, greater comfort, management of different positions, and objective follow-up data. Some have FDA approval and comparative studies against other OSA therapies74–76.
Bignold et al.10 evaluated a vibratory device for POSA treatment in 15 patients using a crossover design and found a significant reduction in supine time and AHI (from 25 to 13.7 events/h). Ravesloot et al.27 showed that a PRT device reduced total AHI and supine time during sleep in 31 POSA patients 4 weeks into therapy, with improved EDS and sleep quality. These findings were corroborated at 6 months by van Maanen69 and more recently in a randomized controlled trial by Laub et al. in 52 POSA patients72.
Levendowski et al.11 demonstrated in 30 POSA patients a reduction in AHI from 24.7-14.7 events/h to 7.5-7.7 events/h (p < .00001) after 4 weeks using a vibratory neck device. The study also showed that PT significantly reduced sleep-disordered breathing and improved sleep quality, while moderately reducing symptoms across OSA severity groups.
Hidalgo Armas et al.77, in a prospective observational interventional study using a forehead vibratory device (n = 128), evaluated multiple parameters over 12 weeks and found a significant reduction in AHI from 30.6 to 20.4 events/h (p < .001), along with reduced supine time, increased total sleep time, and increased N3 and REM sleep. Overall, PRT improves multiple parameters such as AHI, supine time, quality of life, and EDS in POSA patients, with adherence superior to conventional PT, showing adherence rates of 92.7% at 1 month, 89% at 3 months, 64.4% at 6 months, and 82% at 12 months72,73.
Srijithesh et al.78, in a randomized noninferiority crossover trial (n = 40), compared a PRT device (Night Shift) with auto-adjusting continuous positive airway pressure (auto-CPAP) over 16 weeks, crossing treatments at 8 weeks. The primary outcome was EDS; patient treatment preference and PSG parameters were secondary outcomes. The trial was inconclusive because EDS did not meet the predetermined noninferiority margin. Patients preferred auto-CPAP (60%) over PRT (20%), and 20% preferred neither. Residual AHI was lower with CPAP than with PRT (0 ± 3.2 vs 13.0 ± 13.8 events/h, respectively; p = .001).
These findings are consistent with those of Berry et al.79, who included 117 patients and found that while sleep architecture was similar for both treatments (APAP and the medical device used for PRT), microarousals were fewer in the PRT arm, whereas AHI was lower in the APAP arm (AHI, 7.29 vs 3.71), with better oxygen saturation. Notably, the difference in AHI was anticipated in both studies, and overall the relative efficacy of PRT devices was similar to CPAP, maintaining AHI < 10 events/h.
Benoist et al.74 published results from a multicenter randomized prospective controlled trial comparing a MAD with a medical device used for PRT in patients with mild to moderate POSA. A total of 99 patients were randomized to MAD or PRT, and 81 completed the 3-month follow-up. Three months into therapy, no significant differences were observed in AHI (PRT, 13.0 to 7.0 events/h; MAD, 11.7 to 9.1 events/h). Mean adherence was higher with PRT (88.4% vs 60.5%). The authors concluded that both treatments are comparable in effectiveness and adherence in mild to moderate POSA. Importantly, MAD users reported more adverse effects during follow-up vs PRT users (26.8% vs 13.4%), which is relevant given that MAD is increasingly viewed as a temporary therapy due to potential adverse effects on occlusion and dental health.
Some studies have evaluated PRT as combination therapy with MAD or after surgical management of OSA in POSA patients79,80. These suggest additional applications of PRT, but evidence is currently insufficient to draw conclusions; this remains an area for further study.
Finally, AlQarni et al., in a systematic review and meta-analysis, identified 1,119 studies, of which 18 met inclusion criteria (10 randomized controlled trials and 8 cohort studies). Vibrotactile PT significantly reduced AHI at follow-up vs baseline (mean difference, -9.19 events/h; 95% CI, -11.68 to -6.70; p < .00001). The percentage of time in the supine position (%T supine) also dropped significantly (mean difference, -32.79%; 95% CI, -38.75 to -26.83; p < .00001). Percent changes in AHI and %T supine were 43% and 70%, respectively. Secondary endpoints included daytime sleepiness, quality of life, and sleep indices, showing minimal changes, although follow-up was short. The authors concluded that vibrotactile PT was effective in reducing time spent supine and OSA severity, as well as daytime sleepiness; however, the latter did not reach statistical significance81.
Conclusions
POSA is highly prevalent among patients with OSA, regardless of AHI severity. PT and PRT represent an opportunity for stand-alone treatment or as adjunct therapy and have gained acceptance among patients and clinicians due to their efficacy, versatility, and comfort. Nevertheless, more studies are still needed to support their safety and efficacy.
Funding
No specific funding from public-sector agencies, commercial entities, or nonprofit organizations was received for this work.
Conflicts of interest
The authors declared no conflicts of interest whatsoever.
Ethical considerations
Protection of persons and animals. The authors declare that no experiments in humans or animals were performed for this research.
Confidentiality, informed consent, and ethical approval. The authors obtained Ethics Committee approval for analysis of routinely collected and anonymized clinical data; therefore, informed consent was not required. Relevant recommendations were followed.
Declaration on the use of artificial intelligence. The authors declare that they did not use any type of generative artificial intelligence in drafting this manuscript.
