Introduction
Pectus excavatum is a common condition, occurring in up to 1 in 400 children1. Patients requiring surgical treatment should be selected according to symptom severity and radiologic findings2–4. The minimally invasive technique proposed and developed by Nuss in 1987 and published in 1998 is increasingly used5. However, complications may occur, some of which can be severe and potentially life-threatening; therefore, multiple modifications have been proposed to prevent them6–8. Cardiac or vascular injuries, when they occur, usually happen during the creation of a retrosternal tunnel8,9.
This is commonly performed with the Lorenz bar introducer, which achieves only limited mediastinal dissection and involves relatively uncontrolled movements. To obtain a wider dissection, Maryland-type dissectors or an endoscopic Kittner dissector have been used10,11.
To achieve an extensive dissection, the harmonic scalpel appears ideal, as it is an instrument that safely uses ultrasonic energy to allow tissue dissection – similar to the Maryland dissector – but with the advantage of simultaneously separating, cutting, and coagulating tissues.
On the other hand, near-infrared fluorescence has proven useful for delineating anatomic and vascular structures during laparoscopic and robotic surgery, facilitating dissection and making complex procedures safer12,13.
Pediatric reports using this dye are scarce, and there are no publications describing its use during the Nuss procedure14,15.
Damage to the internal mammary artery or intercostal vessels have been reported in this surgery; therefore, the use of this type of dye may allow identification and preservation of these vascular structures8–11.
The aim of this study was to demonstrate the usefulness of the harmonic scalpel used in combination with indocyanine green to facilitate a wide and safe mediastinal dissection during Nuss surgery.
Method
We conducted this prospective, descriptive, observational case series after approval from Hospital Star Médica Infantil Privado Research Committee (Mexico City, Mexico). Inclusion criteria were patients aged 10 to 20 years with pectus excavatum and a Haller index > 3.2 who underwent Nuss repair. Exclusion criteria included patients with deformities other than pectus excavatum or mixed chest wall deformities, those with a Haller index < 3.2, and patients > 20 years. All patients underwent cardiovascular evaluation, pulmonary function testing, plain chest computed tomography, complete blood count, and coagulation studies.
Surgical technique
Patients were placed in the supine position on a 12-cm-high cushion extending from the head to the waist, with the arms positioned alongside the body. For surgical planning, the deepest point of the pectus deformity and the highest points of the anterior chest wall were marked. At this level, a 3-cm incision was performed on both sides along the midaxillary line for dissection and bar insertion.
The harmonic scalpel (Harmonic 1100 Shears; Ethicon, United States) was introduced through the same incision without a trocar. At the level of the midaxillary line, 3 or 4 intercostal spaces above this incision, a 5-mm trocar was inserted, with insufflation set at 5 mmHg at 1 L/min. An initial exploration was performed, and 2 steel sutures were placed at the deepest portion of the sternum and connected to a crane hook to elevate the sternum (Easy Crane system; Primemed, Seoul, South Korea).
Dissection began with the harmonic scalpel at the deepest point of the sternum. At this stage, indocyanine green was administered intravenously at a dose of 1 mg/kg to enable vascular identification. Dissection continued until the left hemithorax was visualized, and the window was widened to allow placement of 2 bars(Figs. 1 A–D). Afterwards, the dissector was advanced to identify the intercostal space of the left hemithorax, visualizing the intercostal vessels. After shaping the lower bar, it was inserted into the intercostal space corresponding to the deepest point. The same maneuver was repeated in the upper intercostal space, inserting a second previously shaped parallel bar (modified Parks pectus bar; Primemed, Seoul, South Korea). Both bars were secured to a stabilizing bridge on each side (Stabilizer-Bridge Fixator; Pampamed, Seoul, South Korea). Hemostasis was verified, the pneumothorax was evacuated, incisions were closed, and a control radiograph was obtained. Pain was managed with cryoanalgesia, serratus muscle block, and dual analgesic therapy. The following data were analyzed: age, sex, cardiovascular evaluation, pulmonary function tests, Haller index, associated morbidity, type of pectus excavatum, operative time, blood loss, residual pneumothorax, hospital stay, patient satisfaction, and other complications.
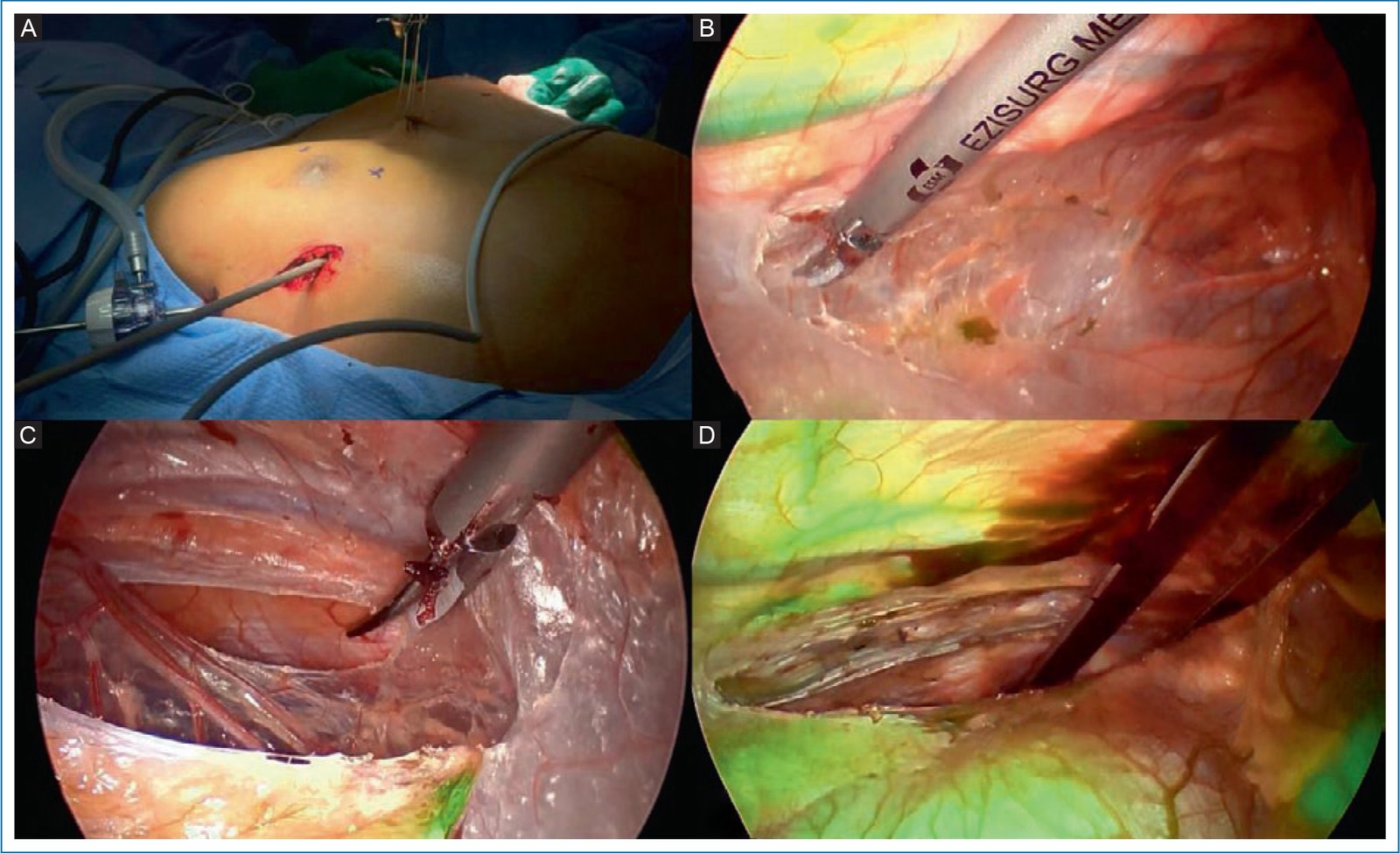
Figure 1. A: introduction of the harmonic scalpel through the same right-sided incision where the bars will be placed. B: initial retrosternal dissection; internal mammary vessels stained with indocyanine green are visible. C: complete dissection to the left side of the chest. D: bar placed through a wide window, preserving chest wall vessels.
Results were analyzed using descriptive statistics.
Results
Between June 2023 and December 2024, a total of 18 patients were treated, aged 11 to 20 years (x̄–: 15.05 years), with a weight ranging from 37 to 67 kg (mean, 47.72 kg); 15 were men and 3 were women. The Haller index ranged from 3.8 to 6.3 (mean, 4.9). Four patients had right-sided asymmetry, 3 left-sided asymmetry, and the remainder had symmetric chest deformity. All patients reported poor body image perception due to pectus excavatum; 9 reported pain and 8 reported dyspnea with mild-to-moderate exertion. Six children had a > 2-year history of asthma. One of them had undergone surgery 7 years earlier for a left lung biopsy; pulmonary adhesions were released without vascular or pulmonary injury using the harmonic scalpel. Preoperative echocardiography showed mitral valve prolapse in 8 children; findings were normal in the remainder. Pulmonary function tests were normal in 9 children, showed mild restriction in 4, and moderate restriction in 5. All were treated using the described surgical technique, and 2 parallel bars were placed. Operative time ranged from 65 to 95 minutes (mean, 78.59 minutes). Blood loss ranged from 10 mL to 25 mL (mean, 14.41 mL). In all patients, the internal mammary artery and intercostal vessels were identified. No allergic reactions occurred.
Seven patients received cryoanalgesia, and in the remaining 11 patients, analgesia was provided via serratus muscle block. Two patients developed minimal residual pneumothorax, which was treated with oxygen. One patient presented bar exposure 6 months after surgery. No other complications occurred. Patients were discharged on postoperative day 4. The aesthetic outcome was satisfactory in all patients.
Discussion
The Nuss technique for correction of pectus excavatum is increasingly performed16. Multiple changes to the original technique have been introduced to reduce complications. Creation of the space between the sternum and pericardium is perhaps the step at which the most serious complications may occur8,17. The procedure requires a critical view, meaning that the surgeon must visualize the tip of the dissector at all times and keep the pericardium separated from the sternum. Sternal elevation, achieved in this study using the Crane technique proposed by Park et al., together with the use of a 30-degree scope, allowed continuous visualization of the dissector tip. With an adequate critical view, the next step is safe mediastinal dissection, for which laparoscopic instruments have been used. Hendrickson et al. used a laparoscopic Kittner dissector placed via a 5-mm trocar located at the left midaxillary line to create, by blind dissection, a window that allowed visualization of the contralateral hemithorax11. Unlike what was reported by Hendrickson, in this study the harmonic scalpel was inserted without a trocar through the right side of the chest, using the same incision through which the dissector and bars would be introduced. This allowed dissection from right to left, which is safer because in patients with pectus excavatum the heart is displaced toward the left and lies closer to the chest wall, making left-sided approaches at higher risk for cardiac injury. We observed that the harmonic scalpel allowed retrosternal space dissection similarly to the Maryland or Kittner dissector, but with the added advantage of simultaneous coagulation, which facilitated the creation of a wide window using small, controlled movements until the left side of the chest was visualized. Moreover, it enabled direct-vision insertion of the bars, visualizing the intercostal exit space in all treated cases. Other advantages include the ability to achieve hemostasis and release pulmonary adhesions simultaneously, as occurred in the patient with prior left lung surgery, in whom adhesions were released from the right side of the chest. The use of indocyanine green simultaneously facilitated identification of blood vessels to allow their preservation or coagulation when necessary. No complications related to the use of the harmonic scalpel or administration of indocyanine green were observed.
Conclusions
The combined use of the harmonic scalpel and indocyanine green allows wide, bloodless mediastinal dissection, facilitating safe and complication-free passage of the dissector and Nuss bars.
Funding
This study did not receive specific funding from public agencies, commercial entities, or nonprofit organizations.
Conflicts of interest
The authors declared no conflicts of interest whatsoever.
Ethical considerations
Protection of human and animal subjects. The authors declare that the procedures followed were in accordance with the ethical standards of the responsible human experimentation committee and in compliance with the World Medical Association and the Declaration of Helsinki. Procedures were approved by the institutional Ethics Committee.
Confidentiality, informed consent, and ethical approval. The authors followed institutional confidentiality protocols, obtained informed consent from patients, and received Ethics Committee approval. Recommendations of the SAGER guidelines were followed, according to the nature of the study.
Declaration on the use of artificial intelligence. The authors declare that no generative artificial intelligence was used in the drafting of this manuscript.
